Sociodemographic determinants of digital health literacy: A systematic review and meta-analysis 数字健康素养的社会人口学决定因素:系统评价和荟萃分析
Marta Estrela ^("a,b,c,d, "^(**)", Guilherme Semedo "^(e)", Fátima Roque "^(d,f)", Pedro Lopes Ferreira "^(c,g)", Maria "){ }^{\text {a,b,c,d, }{ }^{*} \text {, Guilherme Semedo }{ }^{e} \text {, Fátima Roque }{ }^{\mathrm{d}, f} \text {, Pedro Lopes Ferreira }{ }^{\mathrm{c}, g} \text {, Maria }} Teresa Herdeiro ^("a "){ }^{\text {a }} 玛尔塔·埃斯特雷拉 ^("a,b,c,d, "^(**)", Guilherme Semedo "^(e)", Fátima Roque "^(d,f)", Pedro Lopes Ferreira "^(c,g)", Maria "){ }^{\text {a,b,c,d, }{ }^{*} \text {, Guilherme Semedo }{ }^{e} \text {, Fátima Roque }{ }^{\mathrm{d}, f} \text {, Pedro Lopes Ferreira }{ }^{\mathrm{c}, g} \text {, Maria }} ·特蕾莎·赫代罗 ^("a "){ }^{\text {a }}^(a){ }^{\mathrm{a}} iBiMED—Institute of Biomedicine, Department of Medical Sciences, University of Aveiro, Aveiro, Portugal ^(a){ }^{\mathrm{a}} iBiMED—阿威罗大学医学系生物医学研究所,葡萄牙阿威罗^(b){ }^{\mathrm{b}} Department of Social, Political and Territorial Sciences, University of Aveiro, Portugal ^(b){ }^{\mathrm{b}} 葡萄牙阿威罗大学社会、政治和领土科学系^("c "){ }^{\text {c }} Centre for Health Studies and Research, University of Coimbra, Coimbra, Portugal ^("c "){ }^{\text {c }} 科英布拉大学健康研究与研究中心,葡萄牙科英布拉^(d){ }^{\mathrm{d}} Health Sciences Research Center, University of Beira Interior (CICS-UBI), Covilhã, Portugal ^(d){ }^{\mathrm{d}} 贝拉内政大学健康科学研究中心 (CICS-UBI),葡萄牙 Covilhã^(e){ }^{\mathrm{e}} Medical Devices Department, Critical Catalyst, Matosinhos, Portugal ^(e){ }^{\mathrm{e}} Critical Catalyst 医疗器械部,葡萄牙马托西纽什^(f){ }^{\mathrm{f}} Research Unit for Inland Development, Guarda Polytechnic Institute (UDI-IPG), Guarda, Portugal ^(f){ }^{\mathrm{f}} 葡萄牙瓜尔达 瓜尔达理工学院 (UDI-IPG) 内陆发展研究单位^(g){ }^{\mathrm{g}} Faculty of Economics, University of Coimbra, Coimbra, Portugal ^(g){ }^{\mathrm{g}} 科英布拉大学经济学院,葡萄牙科英布拉
A R T I C L E I N F O
Keywords: 关键字:
Digital health literacy 数字健康素养
Systematic Review 系统评价
Digital Health 数字健康
Meta-analysis Meta 分析
Sociodemographic 社会人口统计学
Social Inequalities 社会不平等
Abstract 抽象
Introduction: Differences in digital health literacy levels are associated with a lack of access to digital tools, usage patterns, and the ability to effectively use digital technologies. Although some studies have investigated the impact of sociodemographic factors on digital health literacy, a comprehensive evaluation of these factors has not been conducted. Therefore, this study sought to examine the sociodemographic determinants of digital health literacy by conducting a systematic review of the existing literature. Methods: A search of four databases was conducted. Data extraction included information on study characteristics, sociodemographic factors, and the digital health literacy scales used. Meta-analyses for age and sex were conducted using RStudio software with the metaphor package. Results: A total of 3922 articles were retrieved, of which 36 were included in this systematic review. Age had a negative effect on digital health literacy ( B=-0.05,95%CI[-0.06;-0.04]\mathrm{B}=-0.05,95 \% \mathrm{CI}[-0.06 ;-0.04] ), particularly among older adults, whereas sex appeared to have no statistically significant influence among the included studies ( B=-0.17,95%CI\mathrm{B}=-0.17,95 \% \mathrm{CI} [-0.64; 0.30]). Educational level, higher income, and social support also appeared to have a positive influence on digital health literacy. Discussion: This review highlighted the importance of addressing the digital health literacy needs of underprivileged populations, including immigrants and individuals with low socioeconomic status. It also emphasizes the need for more research to better understand the influence of sociodemographic, economic, and cultural differences on digital health literacy. Conclusions: Overall, this review suggests digital health literacy is dependent on sociodemographic, economic, and cultural factors, which may require tailored interventions that consider these nuances. 简介:数字健康素养水平的差异与缺乏获得数字工具、使用模式和有效使用数字技术的能力有关。尽管一些研究调查了社会人口因素对数字健康素养的影响,但尚未对这些因素进行全面评估。因此,本研究试图通过对现有文献进行系统回顾来检查数字健康素养的社会人口学决定因素。方法: 对 4 个数据库进行了检索。数据提取包括有关研究特征、社会人口学因素和所使用的数字健康素养量表的信息。使用带有隐喻包的 RStudio 软件进行年龄和性别的荟萃分析。结果: 共检索到 3922 篇文章,其中 36 篇被纳入本系统评价。年龄对数字健康素养有负面影响 ( B=-0.05,95%CI[-0.06;-0.04]\mathrm{B}=-0.05,95 \% \mathrm{CI}[-0.06 ;-0.04] ),尤其是在老年人中,而性别在纳入的研究中似乎没有统计学意义 ( B=-0.17,95%CI\mathrm{B}=-0.17,95 \% \mathrm{CI} [-0.64; 0.30])。教育水平、较高的收入和社会支持似乎也对数字健康素养产生了积极影响。讨论:本综述强调了解决贫困人群(包括移民和社会经济地位低下的个人)的数字健康素养需求的重要性。它还强调需要进行更多研究,以更好地了解社会人口、经济和文化差异对数字健康素养的影响。 结论:总体而言,本综述表明数字健康素养取决于社会人口、经济和文化因素,这可能需要考虑这些细微差别的定制干预措施。
1. Introduction 1. 引言
The development of electronic health records and telemedicine has led to an increasing use of digital health tools, gaining significant momentum in the 2000s with the widely available internet [1]. Today, the use of digital health tools has expanded to include health-related apps, wearable devices, and online medical resources to help people manage their health and make informed decisions about health care. The 电子健康记录和远程医疗的发展导致数字健康工具的使用越来越多,在 2000 年代随着互联网的广泛普及而获得了显着的发展势头 [1]。如今,数字健康工具的使用已经扩展到包括与健康相关的应用程序、可穿戴设备和在线医疗资源,以帮助人们管理自己的健康并做出有关医疗保健的明智决策。这
growing use of digital tools in the modern world requires quick adaptation, which is ultimately hindered or facilitated by access to new technologies and the skills needed for their adequate use [2,3]. As the proper use of digital health tools, also known as e-health or eHealth tools, demands a vast number of skills, including numeracy, science literacy, technology use, health literacy, and the capacity to critically appraise health information [4], exploring the digital health literacy context constitutes a complex challenge. 在现代世界,数字工具的日益广泛使用需要快速适应,而获得新技术和充分使用这些技术所需的技能最终会阻碍或促进这种适应[2,3]。由于正确使用数字健康工具(也称为电子健康或电子健康工具)需要大量技能,包括计算能力、科学素养、技术使用、健康素养以及批判性地评估健康信息的能力 [4],因此探索数字健康素养背景构成了一项复杂的挑战。
Digital health literacy is defined as the ability to find, understand, and use health information from digital sources [5], such as the Internet and mobile devices, and is strongly related to the frequency with which people use different health and digital resources. These resources include online video consultations, digital health records, social networks, and other health-related applications aimed at promoting and improving patient health [6]. The burden of digital health illiteracy is significant, as those with difficulty navigating health information may be more vulnerable to misinformation [7]. Differences in digital health literacy levels between individuals persist noticeably, as well as in their online skills and Internet knowledge, which are ultimately related to socioeconomic status and autonomy in the use of these tools [8,9], consequently contributing to social health inequalities and poorer health outcomes [10]. 数字健康素养被定义为从数字来源 [5](如互联网和移动设备)查找、理解和使用健康信息的能力,并且与人们使用不同健康和数字资源的频率密切相关。这些资源包括在线视频咨询、数字健康记录、社交网络和其他旨在促进和改善患者健康的健康相关应用程序 [6]。数字健康文盲的负担是巨大的,因为那些难以浏览健康信息的人可能更容易受到错误信息的影响 [7]。个体之间的数字健康素养水平以及他们的在线技能和互联网知识水平存在显著差异,这最终与社会经济地位和使用这些工具的自主性有关 [8,9],从而导致社会健康不平等和更差的健康结果[10]。
Currently, there are several approaches to address digital inequality. A three-level model for digital divide has been presented by van Deursen & Helsper [3], with the first digital divide level being associated with lack of access to digital tools and the means to access the Internet, the second level to usage patterns, and the last level being associated with the ability to use digital technologies effectively and efficiently to achieve improved outcomes. Nevertheless, digital divide - and each of these levels present on the three-level model - is influenced by factors such as socioeconomic status, generation, sex, region, and health status, with the first being one of the main predictors of Internet access and associated skills, directly influencing competent Internet use [3,11,12]. Furthermore, digital health literacy can be influenced by other factors such as technology readiness, attitudes towards technology, and Internet use patterns [13-16]. Although some studies have reported the influence of sociodemographic factors on digital health literacy, a systematic appraisal of these factors is lacking. Thus, this study aimed to analyze the sociodemographic determinants of digital health literacy through a systematic review and meta-analysis of the available studies on the topic. 目前,有几种方法可以解决数字不平等问题。van Deursen 和 Helsper [3]提出了一个三级数字鸿沟模型,第一级数字鸿沟与缺乏数字工具和访问互联网的方式有关,第二级与使用模式有关,最后一级与有效和高效地使用数字技术以实现改善结果的能力有关。然而,数字鸿沟——以及三级模型中存在的每一个水平——都受到社会经济地位、世代、性别、地区和健康状况等因素的影响,其中第一个因素是互联网访问和相关技能的主要预测因素之一,直接影响互联网的有效使用[3,11,12]。此外,数字健康素养还可能受到其他因素的影响,例如技术准备情况、对技术的态度和互联网使用模式 [13-16]。尽管一些研究报告了社会人口学因素对数字健康素养的影响,但缺乏对这些因素的系统评估。因此,本研究旨在通过对有关该主题的现有研究进行系统评价和荟萃分析,分析数字健康素养的社会人口学决定因素。
2. Methods 2. 方法
2.1. Screening and study selection 2.1. 筛选和研究选择
A search was conducted on November 24, 2021, on MedLINEPubMed, Scopus, Web of Knowledge, and EMBASE databases. To update the results obtained, a new search was conducted on April 12, 2022, using the same databases. The screening of the obtained articles was conducted by title and abstract by two independent researchers (ME and GS), and the search strategy was primarily designed to identify relevant studies that analyze the influencing factors on digital health literacy, and identify which scales were used in these studies to measure digital health literacy. The keywords used to search the aforementioned databases are as follows: 于 2021 年 11 月 24 日在 MedLINEPubMed、Scopus、Web of Knowledge 和 EMBASE 数据库中进行了检索。为了更新获得的结果,我们于 2022 年 4 月 12 日使用相同的数据库进行了新的检索。获得的文章由两名独立研究人员 (ME 和 GS) 按标题和摘要进行筛选,检索策略主要旨在确定分析数字健康素养影响因素的相关研究,并确定这些研究中使用了哪些量表来衡量数字健康素养。用于搜索上述数据库的关键字如下:
(digital health OR e-health OR ehealth) AND literacy AND (determinants OR factors OR sociodemographic OR demographic OR scale) (数字健康 OR 电子健康 OR 电子健康)和识字率 AND (决定因素 OR 因素 OR 社会人口统计学 OR 人口统计学 OR 量表)
This systematic review was registered in the PROSPERO database (CRD42022325207) [17]. 该系统评价已在 PROSPERO 数据库 (CRD42022325207) 中注册 [17]。
2.2. Selection criteria 2.2. 选择标准
The inclusion criteria accepted studies that analyzed the influence of sociodemographic factors, such as sex, age, income, geographic region, and social status. There was no time restriction and the languages of the included studies were English, Portuguese, or Spanish. Conference abstracts, systematic reviews, reviews, meta-analyses, editorials, study protocols, scale design and validation studies, correspondence papers, and studies that were not within the scope of our study were excluded. 纳入标准接受了分析社会人口学因素影响的研究,例如性别、年龄、收入、地理区域和社会地位。没有时间限制,纳入研究的语言是英语、葡萄牙语或西班牙语。会议摘要、系统评价、综述、荟萃分析、社论、研究方案、量表设计和验证研究、函授论文以及不属于我们研究范围的研究被排除在外。
All titles and abstracts obtained from the searches were independently reviewed by two researchers. The inclusion and exclusion criteria 从检索中获得的所有标题和摘要均由两名研究人员独立审查。纳入和排除标准
were applied by ME and GS and validated by a third researcher (TH) when there was no agreement. Inter-rater agreement was calculated using the Cohen’s kappa coefficient. Full-text articles were selected using the same approach. 由 ME 和 GS 应用,并在未达成一致时由第三位研究人员 (TH) 验证。评分者间一致性是使用 Cohen 的 kappa 系数计算的。使用相同的方法选择全文文章。
2.3. Quality assessment 2.3. 质量评估
The quality of the included studies was assessed using the Joanna Briggs Institute Checklist for Cross-sectional studies [18]. For each study, the risk of bias was assessed separately by two researchers (ME and GS). Similar to the screening process, a third reviewer (TH) acted as a referee to reach a consensus in case of disagreement. 使用 Joanna Briggs Institute 横断面研究清单 [18] 评估纳入研究的质量。对于每项研究,偏倚风险由两名研究人员 (ME 和 GS) 分别评估。与筛选过程类似,第三位审稿人 (TH) 作为推荐人,在出现分歧时达成共识。
2.4. Data analysis 2.4. 数据分析
Data extraction retrieved information on authors, year, country, study design, study population, response rate, average digital health literacy score, and a brief description of the main digital health literacy determinants, namely sociodemographic characteristics. The primary outcome was the impact of the aforementioned sociodemographic characteristics on digital health literacy levels, and the secondary outcome was the scale used to analyze digital health literacy. The results were summarized qualitatively and quantitatively. This systematic review and meta-analysis followed the PRISMA [19] and MOOSE [20] guidelines. Further recommendations for conducting meta-analyses of observational studies were retrieved from a study by Mueller [21]. 数据提取检索了有关作者、年份、国家、研究设计、研究人群、回复率、平均数字健康素养分数的信息,以及主要数字健康素养决定因素的简要描述,即社会人口学特征。主要结局是上述社会人口学特征对数字健康素养水平的影响,次要结局是用于分析数字健康素养的量表。对结果进行了定性和定量总结。本系统评价和荟萃分析遵循 PRISMA [19] 和 MOOSE [20] 指南。Mueller 的一项研究进一步推荐了对观察性研究进行 meta 分析[21]。
2.5. Statistical analysis 2.5. 统计分析
All statistical analyses were conducted using RStudio software (v. 4.2.2), and the packages metafor [22], dplyr, and readxl. Regression coefficients were estimated with 95%95 \% confidence intervals using a random-effects model with Hedges and Olkin’s estimator [23,24]. Heterogeneity due to differences between studies was assessed using Cochran’s Q and I2-statistic [25,26]. Forest plots were used to visually represent the presence of heterogeneity. Publication bias was assessed using funnel plots [27] - see supplementary figures S2). Sensitivity for age was assessed through subgroup analyses of young adults, adults, and older adults. As there were no evident subgroups for sex, sensitivity analyses for this variable were conducted using the leave-one-out method. 所有统计分析均使用 RStudio 软件 (v. 4.2.2) 以及软件包 metafor [22]、dplyr 和 readxl 进行。使用带有 Hedges 和 Olkin 估计器的随机效应模型 [23,24] 估计回归系数和 95%95 \% 置信区间。使用 Cochran 的 Q 和 I2 统计量评估研究差异引起的异质性 [25,26]。森林图用于直观地表示异质性的存在。使用漏斗图 [27] 评估发表偏倚 - 见补充图 S2)。通过对年轻人、成人和老年人的亚组分析来评估对年龄的敏感性。由于性别没有明显的亚组,因此使用留一法对该变量进行敏感性分析。
3. Results 3. 结果
3.1. Screening 3.1. 筛选
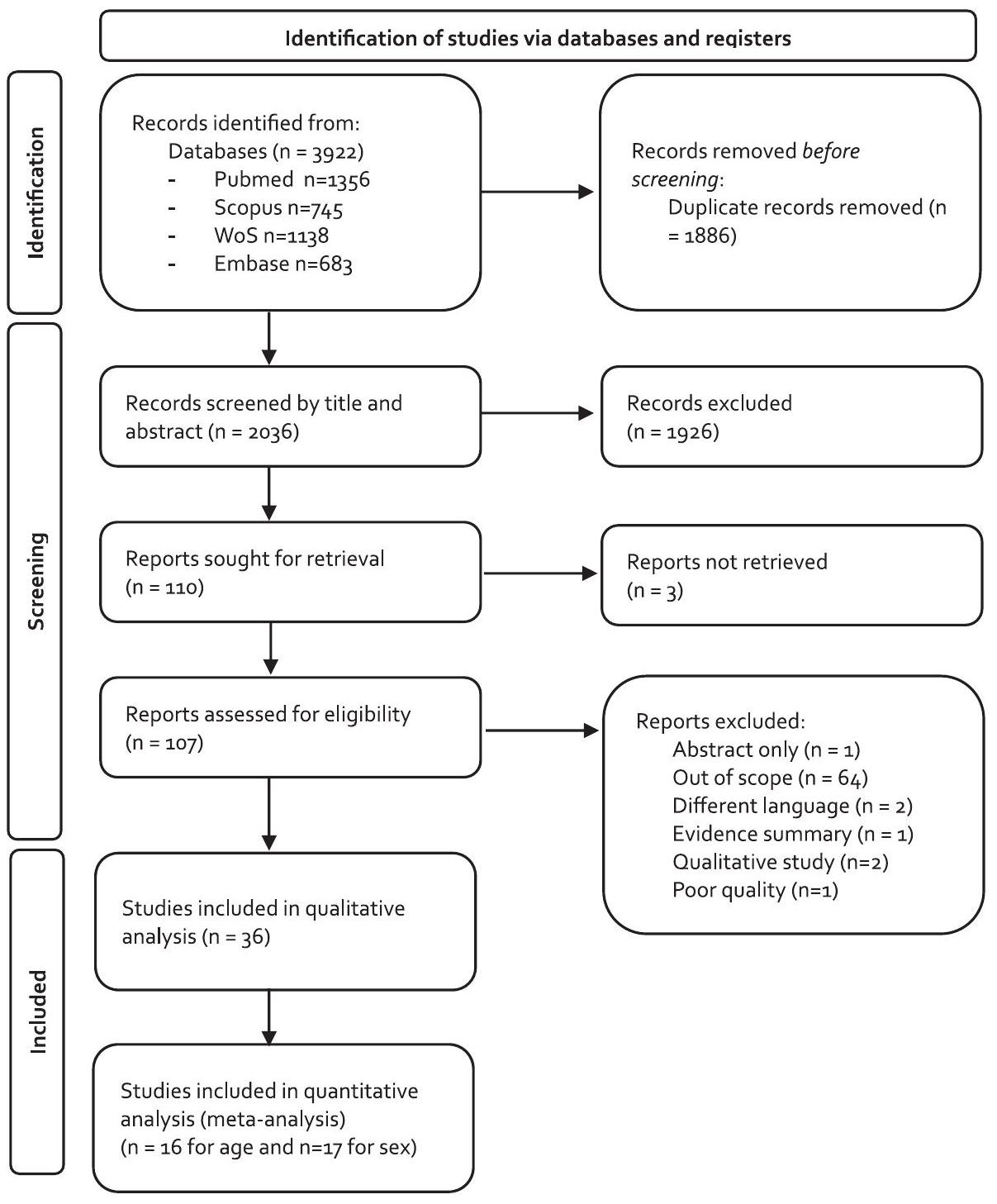
A total of 3922 articles were retrieved from Pubmed, Scopus, WoS, and EMBASE databases, of which 1886 were duplicates (Fig. 1). Screening by title and abstract was conducted, and 1926 records were excluded as they did not agree with the inclusion criteria, achieving a Cohen’s kappa of 0.623 , corresponding to substantial agreement [28]; 110 reports were analyzed by full text to check eligibility. Of these, 36 were included in this systematic review. Cohen’s kappa of 0.861 was obtained, corresponding to an almost perfect agreement [28] between the researchers. 从 Pubmed、Scopus、WoS 和 EMBASE 数据库中共检索到 3922 篇文章,其中 1886 篇是重复的(图 1)。按标题和摘要进行筛选,排除了 1926 条记录,因为它们不符合纳入标准,达到了 0.623 的 Cohen κ,对应于基本一致性 [28];对 110 份报告进行了全文分析以检查资格。其中,36 例被纳入本系统评价。获得了 0.861 的 Cohen κ,对应于研究人员之间几乎完美的一致性 [28]。
3.2. Quality analysis 3.2. 质量分析
The quality analysis was conducted by two independent researchers. From the thirty-seven studies included after full-text screening, one study was removed for inadequate reporting of results. Although the remaining studies had overall good quality, some criteria were classified as “unclear” for some studies, especially regarding inclusion criteria of the sample, exposure measurement, and confounding factor identification/management. The results of the quality analysis are shown in supplementary material - Table S2. 质量分析由两名独立研究人员进行。在全文筛选后纳入的 37 项研究中,1 项研究因结果报告不充分而被删除。尽管其余研究总体质量良好,但一些研究的一些标准被归类为 “不清楚”,特别是在样本的纳入标准、暴露测量和混杂因素识别/管理方面。质量分析的结果显示在补充材料 - 表 S2 中。
All studies used the eHealth Literacy Scale (eHEALS), except for Zakar’s study [29], which used the Digital Health Literacy Instrument. The weighted average eHEALS score among the studies was 30.4+-2.430.4 \pm 2.4. Table 1 presents the main characteristics of the studies included. The data extracted from the regression analyses are presented in Table S1. 所有研究都使用了电子健康素养量表 (eHEALS),除了 Zakar 的研究 [29] 使用了数字健康素养工具。研究中的加权平均 eHEALS 评分为 30.4+-2.430.4 \pm 2.4 。表 1 列出了所纳入研究的主要特征。从回归分析中提取的数据如表 S1 所示。
Table 2 summarizes the characteristics analyzed in each study. Almost all the studies analyzed age and sex. The results of the effect of each variable on digital health literacy scores are included in the supplementary material. 表 2 总结了每项研究中分析的特性。几乎所有的研究都分析了年龄和性别。每个变量对数字健康素养分数的影响结果包含在补充材料中。
3.4. Study design and setting 3.4. 研究设计和设置
All studies had a cross-sectional design. Seventeen studies were conducted on-site [13,16,30-44], either through interviews or the distribution of a questionnaire; nine studies were conducted online [29,45-52], and five studies were conducted through telephone (CATI) [53-57]. The remaining five studies adopted a mixed approach [58-62], using two of the aforementioned data collection strategies. 所有研究均采用横断面设计。17 项研究是通过访谈或分发问卷进行现场进行的[13,16,30-44];9 项研究通过在线进行[29,45-52],5 项研究通过电话(CATI)进行[53-57]。其余 5 项研究采用混合方法[58-62],使用了上述两种数据收集策略。
3.5. Location 3.5. 位置
The included studies are distributed around the globe: almost half of the studies (14//36)(14 / 36) were conducted in Asian countries [13,29-35,45-48,58,59]. Twelve studies were conducted in North America [16,36-39,49-51,53-55,60][16,36-39,49-51,53-55,60], six in Europe [40,41,56,57,61,62], three in Africa [42,43,52] and one in Australia [44]. 纳入的研究分布于全球:几乎一半的研究 (14//36)(14 / 36) 是在亚洲国家进行的[13,29-35,45-48,58,59]。12 项研究在北美进行 [16,36-39,49-51,53-55,60][16,36-39,49-51,53-55,60] ,6 项在欧洲进行[40,41,56,57,61,62],3 项在非洲进行[42,43,52],1 项在澳大利亚进行[44]。
3.6. Population characteristics 3.6. 种群特征
Seven studies were conducted among high school or college students [29,30,32,35,41,42,47]. Older adults were the target population in six studies [16,31,36,39,49,55], while one study included younger and older adults [59]. Of the remaining twenty-two studies, eight targeted populations with specific diseases [36,43,44,50,51,54,60,61], one targeted at healthcare workers [46], and the remaining had patients in general or the general population as the target population. 7项研究在高中生或大学生中进行[29,30,32,35,41,42,47]。6项研究的目标人群为老年人[16,31,36,39,49,55],1项研究纳入了年轻人和老年人[59]。在其余 22 项研究中,8 项研究针对患有特定疾病的人群 [36,43,44,50,51,54,60,61],1 项针对医护人员 [46],其余研究以一般患者或一般人群为目标人群。
3.6.1. Digital health literacy levels 3.6.1. 数字健康素养水平
From studies that presented average eHEALS scores among respondents, it was observed that healthcare workers [46] and online health consumers [52] presented higher levels of digital health literacy. 从显示受访者平均 eHEALS 分数的研究中观察到,医护人员 [46] 和在线健康消费者 [52] 表现出更高水平的数字健康素养。
Corresponding author at: Department of Medical Sciences, Institute of Biomedicine - iBiMED- University of Aveiro, Campus Universitário de Santiago Agra do Crasto - edifício 30 3810-193 Aveiro, Aveiro, Portugal. 通讯作者:医学科学系,生物医学研究所 - iBiMED- 阿威罗大学,圣地亚哥大学校园 阿格拉杜克拉斯托 - edifício 30 3810-193 Aveiro, Aveiro, Portugal.