
Changes in Cardiac Metabolism in Prediabetes
糖尿病前期心脏代谢的变化

作者:Vera H. W. de Wit-Verheggen 1
马斯特里赫特大学医学中心营养与代谢转化研究学院营养与运动科学系,荷兰马斯特里赫特 6200 MD
马斯特里赫特大学医学中心放射学和核医学系,荷兰马斯特里赫特 6200 MD
应向其发送信件的作者。
生物分子 2021, 11(11), 1680;https://doi.org/10.3390/biom11111680
收到的意见书日期: 2021-10-13 / 修订日期: 2021-10-28 / 录用日期: 2021-11-8 / 出版日期: 2021-11-12
(本文属于特刊《心力衰竭:分子机制与新型治疗方法》)
Abstract 抽象
在 2 型糖尿病 (T2DM) 中,心血管疾病 (CVD) 的患病率增加,即使针对动脉粥样硬化和其他 CVD 危险因素进行了纠正。舒张功能障碍是心力衰竭发作前心脏功能的早期变化之一,它已经发生在糖尿病前期状态。很明显,这些变化与心脏代谢的改变密切相关;然而,确切的病因尚不清楚。在这篇叙述性综述中,我们概述了糖尿病前期脂肪酸和葡萄糖代谢的早期心脏变化及其对心脏功能的影响。更好地了解代谢、线粒体功能和心脏功能之间的关系将有助于深入了解糖尿病前期心功能下降的病因。
关键词:心脏代谢;糖尿病前期;线粒体功能;心脏功能
1. Introduction 1. 引言
糖尿病前期定义为空腹血糖受损(空腹血糖在6.1-6.9 mmol/L之间)或葡萄糖耐量受损(2小时血浆葡萄糖在7.8-11.0 mmol/L之间)[1],使个体处于发生2型糖尿病(T2DM)及其心血管疾病(CVD)相关并发症的高风险中[2,3]。心血管疾病风险的增加与糖尿病前期的空腹血糖成正比[2,4,5],主要由动脉粥样硬化引起,由糖尿病前期患者特有的许多危险因素诱发,例如血脂异常和高血压[6,7,8,9,10,11,12]。动脉粥样硬化导致缺血性心脏病在既往文献中已有广泛讨论[13]。然而,即使对动脉粥样硬化、胆固醇值、体重、血压和年龄进行校正,糖尿病前期患者发生心力衰竭的风险仍然增加,主要是由于舒张功能障碍(在T2DM中称为糖尿病性心肌病(diabetic cardiomyopathy, DCM))[14,15]。这种现象也属于射血分数保留的心力衰竭(heart failure with preserved ejection fraction, HFpEF)[16]。
有趣的是,舒张功能障碍不仅存在于T2DM中,也存在于糖尿病前期[17]。有证据表明,在糖尿病前期患者中,较高的血糖水平与较低的心功能参数相关[ 17],表明心脏功能的变化出现在T2DM发生的早期。高血糖反应的心脏代谢变化被认为是T2DM引起DCM的重要途径[18,19],这可能已经在糖尿病前期发挥作用。识别这些代谢变化可能有助于更好地了解糖尿病前期舒张功能障碍的潜在病因,这为在 T2DM 早期发展中预防 DCM 提供了机会之窗。因此,本叙述性综述将仅关注糖尿病前期心脏功能下降背后的可能心脏代谢机制(无论其CVD风险状况如何),因为这些变化发生在DCM发病之前。我们不会讨论其他可能的途径,如氧化应激和炎症,也不会讨论DCM [ 20, 21, 22],这些途径已经在文献中被广泛讨论。
2. Cardiac Fat 2. 心肌脂肪
当能量摄入超过消耗时,最终会导致体内脂肪堆积,这在肥胖症中可见[23]。大量过剩的营养物质还会导致脂肪组织以外的器官(如骨骼肌、肝脏和心脏)中脂肪沉积。这种异位脂质积累与许多组织的胰岛素抵抗有关。因此,心脏脂肪堆积可能在糖尿病前期心脏舒张变化的发展中起重要作用。心脏脂质含量可以通过体内和体外方法进行研究。
体内研究使用磁共振波谱 (MRS) 对参与脂质代谢的代谢物进行相对定量。质子MRS( 1 H-MRS)产生一个光谱,其中可以区分多个脂质信号(CH 2 和CH 3 ),肌酸(Cr)信号和水(H 2 O)信号。CH 2 /H 2 O通常用作反映心肌甘油三酯含量的参数,这主要代表心肌中甘油三酯的中性脂质储存。通过这种体内技术,结果表明,与瘦个体相比,超重和肥胖个体的心肌甘油三酯含量增加[24],糖尿病前期和T2DM患者的心肌甘油三酯含量可能更高[25]。此外,心肌甘油三酯含量与胰岛素敏感性呈弱相关,由稳态模型评估指标确定[25]。
体外研究发现,与瘦患者相比,代谢综合征(平均HOMA评分4.±2分,标准差0.5,标准差0.5)患者的心肌内脂质沉积增加[26]、肥胖或T2DM[27]。此外,Anderson等人发现,在非糖尿病患者和糖尿病患者中,心脏脂肪含量与HbA1c呈正相关[28]。这些离体研究表明,与健康的瘦人相比,糖尿病前期个体的心脏脂肪增加[26,27,28],这与McGavock等人[25]的上述体内结果一致。
有趣的是,已经描述了心脏脂肪堆积和心脏功能之间的几个联系。Van der Meer等人发现,在葡萄糖代谢正常(NGM)的瘦个体中,通过 1 H-MRS测量的心肌甘油三酯含量增加(在极低热量饮食后)与舒张功能下降相关[29]。此外,在代谢综合征(HOMA评分高)的个体中,发现心脏脂肪堆积量与心功能障碍进展(通过心肌功能指数和射血分数测量)之间存在相关性[26]。与瘦个体相比,超重和肥胖个体的心肌甘油三酯含量增加伴有左心室肿块升高和间隔壁增厚抑制[24]。这表明,可能在糖尿病前期,心脏脂肪储存的增加可能会对心脏功能产生负面影响。
3. Adipose Tissue Surrounding the Heart
3. 心脏周围的脂肪组织
心脏周围的脂肪沉积(心外膜脂肪组织和心包脂肪组织)通常也会随着超重/肥胖而增加,据报道在糖尿病患者中更为明显。这些库尚未在糖尿病前期人群中进行特异性测量,尽管缺乏这些单独库在糖尿病前期的具体数据,但可以预期,由于糖尿病前期心脏脂肪增加,并且健康男性的心脏脂肪厚度与心脏脂肪密切相关,因此可以预期心外膜脂肪组织(EAT)在糖尿病前期升高[30]。然而,需要定量研究来证实糖尿病前期个体的这一概念。
从肥胖个体中可以知道,当EAT扩张时,脂肪酸的储存和释放之间的平衡会转向更活跃的分泌[31]。此外,扩增的EAT将其分泌谱转变为更促炎的细胞因子和趋化因子,对邻近细胞产生负面影响[32,33,34]。这导致慢性炎症反应,显示存在于扩大的EAT组织中[35,36]。此外,炎症介质的这种局部分泌也可以抑制胰岛素的活性。事实上,EAT与胰岛素抵抗和代谢综合征呈正相关[37,38]。
文献表明,EAT的扩张对心脏功能有负面影响[39,40,41]。尽管缺乏对糖尿病前期 EAT 的研究,但 EAT 增加对功能参数的不利影响似乎是一种普遍现象,并且在瘦、肥胖和 T2DM 个体中都有报道。首先,从长轴视图测量的心包脂肪厚度被证明是左心室外侧壁(称为e'外侧)活动性的预测因子[39]。其次,病态肥胖个体的EAT厚度与心房扩大和右心室和左心室舒张期充盈受损有关[42]。这与平均BMI正常但代谢综合征和T2DM患病率较高的健康人群的研究结果一致,其中PF体积与左心房直径和E/e'相关[41]。在病态肥胖的女性个体中,左心室周围的脂肪组织体积不仅与舒张功能参数(峰值早期充盈速度(E)和峰值晚期充盈速度(A))相关,还与一些左心室血流动力学测量值相关,包括心输出量和每搏输出量[40]。此外,EAT与左心室质量(left ventricular mass, LVM)相关,左心室质量是心血管不良结局的强预测因子[31,41]。
EAT与心脏功能之间的关联可以通过多种机制来解释。首先,EAT是FFA的储存库,因此可以为心脏提供营养[32],从而促进心脏脂质代谢的改变。其次,慢性炎症反应(显示存在于扩大的EAT组织中)[35,36],以及EAT产生的炎性细胞因子可能在局部起作用,作为旁分泌动脉粥样硬化因子[32]。最后,机械性障碍可能会限制心肌的扩张性[43]。
由于缺乏关于EAT与心脏代谢和功能变化关系的研究,因此需要更多的研究。特别是因为众所周知,EAT更灵活,甚至在心脏脂肪减少之前就减少了[44]。EAT可能导致糖尿病前期的舒张功能障碍;然而,在多大程度上仍有待阐明。
4. Enhanced Cardiac Lipid Metabolism
4. 增强心脏脂质代谢
胰岛素通常抑制脂肪分解,从而减少血浆非酯化脂肪酸 (NEFA) 的释放。然而,在胰岛素敏感性降低的个体中,如糖尿病前期的情况,胰岛素的餐后效果受损,使循环游离脂肪酸(ffa)升高[45]。除了循环中 FFA 水平增加外,PET 研究表明,糖尿病前期心肌中的 FFA 摄取和 FFA 氧化都增加。Labbé等人使用 18 F-氟-6-硫杂七烷酸(FTHA)作为脂肪酸示踪剂和[ 11 C]乙酸盐来测定心脏灌注和氧化代谢指数,结果显示,与葡萄糖代谢(NGM)正常的个体相比,糖尿病前期个体(定义为葡萄糖耐量受损)在心脏中吸收增加,餐后前6小时心肌氧化代谢增加[46]。这与肝脏和骨骼肌中脂肪酸的摄取形成鲜明对比,因为与餐后状态的NGM相比,这些脂肪酸在糖尿病前期仍然相似[46]。Brassard 等人证实了这些关于血浆中 FFA 可用性增加和心肌 FFA 代谢的发现,与 T2DM 风险不增加的匹配个体相比,T2DM 个体的血糖正常一级亲属(因此患 T2DM 的风险高度增加)。 使用稳定同位素示踪剂([1,1,2,3,3-H 2 5 ]-甘油和[U-C 13 ]-棕榈酸酯或[1,2-C 13 ]-乙酸酯),他们发现,在高胰岛素水平下血管内TG溶脂增强期间,这些T2DM高危个体的NEFA血浆外观增加,NEFA心肌氧化增加[45]。
Brassard和Labbé在胰岛素刺激条件下的这些发现指出,在糖尿病前期,心脏脂肪酸处理已经发生了变化,与NGM相比,心脏中脂肪酸的摄取和氧化增加。此外,Labbé等人发现,脂质代谢的这些变化可能是心脏功能的适应不良。糖尿病前期患者NEFA摄取和氧化的增加与左心室射血分数(LVEF)降低、左心室每搏输出量减少以及舒张功能受损有关[46]。这与Mather等人在T2DM个体中的研究结果一致,他们表明,在空腹和胰岛素治疗条件下(通过16-[ 18 F]氟-4-硫酰棕榈酸酯(FTP)和 11 C-乙酸酯测量)的心肌脂肪酸氧化增强伴有心脏工作效率降低[47]。这可能不足为奇,因为以牺牲碳水化合物氧化为代价增加脂肪酸氧化会增加需氧量,导致心肌效率降低[47]。此外,在已知动脉粥样硬化风险增加的糖尿病前期个体中,这使得心脏更容易缺血。因此,糖尿病前期脂肪酸代谢的增强对收缩能力和缺血耐受性有影响[47]。
抵消这种改变的底物代谢以预防 T2DM 中的 DCM 可能是有益的。糖尿病前期心脏早期发生的代谢变化似乎是可逆的,正如糖尿病前期个体的几项研究表明的那样。减肥手术后六个月,糖尿病前期患者全身胰岛素敏感性有所改善,这与心肌空腹游离脂肪酸摄取的减少呈正相关,也与心肌功能呈正相关。虽然心脏脂肪没有减少,但心肌结构得到改善[44]。Labbé等人在糖尿病前期中观察到类似的结果,在1年的生活方式干预后,适度的体重减轻导致底物代谢的变化和心脏功能的改善[48]。然而,糖尿病前期7天的短期饮食并不能改善心脏功能[49],因此表明心脏代谢和功能的结构变化需要更长的时间才能发展。
5. Decreased Cardiac Glucose Metabolism
5. 心脏葡萄糖代谢降低
随着心脏脂肪酸代谢的改变,糖尿病前期的心脏葡萄糖代谢可能会发生相互变化[50]。在这里,使用葡萄糖类似物 [ 18 F]-氟脱氧葡萄糖 ( 18 F-FDG) 的 PET 研究可以深入了解葡萄糖的心肌摄取。Kim等人研究了NGM、糖尿病前期和T2DM的混合人群,发现内脏脂肪区和空腹FFA是空腹条件下心肌葡萄糖摄取的独立决定因素[51]。然而,Kim等人和胡等人都表明,在空腹条件下,糖尿病前期与心肌葡萄糖摄取减少无关,而T2DM为[51,52],这与动物研究一致[53]。然而,在进食或胰岛素刺激状态下,结果可能有所不同。
与Kim等人研究中的禁食个体相比,Nielsen等人研究了NGM、糖尿病前期和新诊断的T2DM个体在口服葡萄糖摄入后1小时的心肌葡萄糖摄取,这些个体的特征都是慢性心力衰竭和LVEF降低。尽管心肌血流量和心肌血流量储备相似,但与NGM相比,糖尿病前期和新诊断的T2DM患者尽管葡萄糖和胰岛素水平升高,但心肌葡萄糖摄取量降低[54]。然而,由于作者没有对糖尿病前期和T2DM患者进行单独的分析,因此尚不清楚这些组之间是否存在差异。
为了评估胰岛素刺激的心肌葡萄糖摄取,在比葡萄糖摄入后更可控的情况下,应测量高胰岛素正常血糖钳夹期间的心肌葡萄糖摄取[55]。Eriksson等人在年龄、性别和BMI匹配的对照组、糖尿病前期和T2DM个体中,在这种钳夹期间的心脏葡萄糖代谢率相似[56]。在高胰岛素正常血糖钳夹期间,与(BMI匹配的超重)NGM个体相比,T2DM患者的心肌葡萄糖摄取较低[55,57]。T2DM中心肌葡萄糖摄取的这些相互矛盾的体内发现也在体外研究中发现。T2DM患者左心室的全层心肌活检显示,与NGM超重对照组相比,心脏胰岛素受体底物1(IRS1)–PI 3激酶(PI3K)活性增加[58]。这意味着即使在这种胰岛素抵抗状态下,胰岛素信号级联反应也是完整的。然而,由于离体研究中的所有个体都以左心室功能障碍为特征,因此组间差异可以减弱。
总体而言,糖尿病前期心肌葡萄糖摄取的结果相互矛盾,无论是在体内还是在体外研究中。一些人发现,在禁食状态[51]和钳夹期间[56],与NGM或T2DM个体相比,健康糖尿病前期个体没有差异,而另一些人则发现,在慢性心力衰竭的糖尿病前期患者中,口服葡萄糖负荷后1小时心肌葡萄糖摄取减少[54]。此外,先前的文献尚不清楚在高胰岛素正常血糖钳夹期间测量的心肌葡萄糖摄取是否与全身胰岛素敏感性相关[57][56]。数据分散,问题仍然是糖尿病前期是否以心肌胰岛素敏感性降低为特征。
到目前为止,心肌葡萄糖代谢改变对心脏功能的影响仅在心力衰竭患者中进行了研究。动物研究显示相互矛盾的结果。在糖尿病Zucker大鼠中,葡萄糖使用减少(通过 18 F-FDG作为PET示踪剂评估)与舒张和收缩心脏功能受损(超声评估)有关[53]。令人惊讶的是,一项针对胰岛素抵抗的Sprague-Dawley大鼠的研究表明,心肌的葡萄糖使用增加,伴有较高的左心室射血分数,较小的左心室收缩末期容积和较厚的收缩末期壁厚[59]。因此,其机制尚不清楚,糖尿病前期葡萄糖代谢、胰岛素和心脏功能之间的关系也未被探索。
MRS研究侧重于示踪剂超极化[1-C 13 ]-丙酮酸或[2-C 13 ]-丙酮酸,提供了机制信息,并揭示了PDH水平上碳水化合物代谢的缺陷。尽管使用这种新技术进行的研究很少,但最初的结果是有希望的。Cunningham等人表明,评估人体体内心脏丙酮酸代谢是可行的[60],Rider等人发现,与年龄匹配的健康对照组相比,T2DM中通过心脏丙酮酸脱氢酶的代谢通量显著降低[61]。因此,在 T2DM 中,除了胰岛素抵抗外,通过丙酮酸脱氢酶的代谢通量减少可以解释葡萄糖摄取减少。此外,在口服葡萄糖负荷后,T2DM个体通过丙酮酸脱氢酶的代谢通量显著增加[61]。T2DM个体中丙酮酸脱氢酶的通量降低与各种动物模型的结果一致[62,63,64]。Chatham等人发现,Zucker糖尿病脂肪大鼠[62]和链脲佐菌素诱导的糖尿病的分离灌注大鼠心脏[63]的通量降低。有趣的是,PDH通量与舒张功能有关[63,64]。希望未来使用这种优雅方法的研究可以更深入地了解人类糖尿病前期状态下可能调节葡萄糖和脂肪氧化的潜在机制。
在糖尿病前期状态下发现葡萄糖代谢变化的情况下,这些变化是可逆的,类似于脂质代谢的可能改变。即使在减肥手术和随后的体重减轻后1个月内,严重肥胖的T2DM也显示出心肌葡萄糖摄取的增加[65]。Hannukainen 等人研究了 46 名患有 T2DM、葡萄糖耐量受损和 NGM 的个体,这些个体在减肥手术前和手术后六个月体重减轻。不仅检测到全身胰岛素敏感性的改善,这与心肌葡萄糖摄取的增加和心肌空腹游离脂肪酸摄取的减少呈正相关,而且心肌功能和心肌结构也得到改善[44]。然而,就像对脂质代谢有积极影响的生活方式干预一样,从这项研究中,我们不知道这些变化是否是由于减肥的全身效应。在T2DM和冠状动脉疾病患者中,使用PPARγ受体激动剂罗格列酮进行为期16周的干预,可增加缺血和非缺血区域的高胰岛素正常血糖钳夹期间的心肌葡萄糖摄取[66],表明心肌葡萄糖摄取不仅会受到减肥手术或生活方式调整的影响,还会受到药物的影响。
6. Mitochondrial Function
6. 线粒体功能
线粒体负责氧化代谢,是心肌细胞正常功能的关键。因此,线粒体功能障碍被怀疑在DCM的发展中起关键作用也就不足为奇了[67,68]。不幸的是,该领域缺乏糖尿病前期的人类数据。尽管对高脂肪喂养并接受链脲佐菌素治疗作为糖尿病前期模型的雄性Long-Evans大鼠的研究表明,轻度舒张功能障碍和心脏肥大与线粒体自噬的早期变化有关[69]。这支持了线粒体功能障碍是糖尿病前期 DCM 发展的基础这一观点。
然而,来自肥胖症和 T2DM 体内和体外研究的信息是可用的,可以解释糖尿病前期线粒体功能的可能变化。从使用高分辨率呼吸测量法作为线粒体功能反映的离体研究中,已知较低的线粒体呼吸与T2DM有关[28,70]。这表明,尽管 T2DM 个体更喜欢脂肪酸氧化,但与非糖尿病个体相比,T2DM 个体的心肌偏好脂肪酸支持呼吸的最大能力降低。此外,Anderson等人报道了脂肪酸呼吸的最大能力与HbA1c呈负相关[28]。与 Hb1A1c 的关系可能表明线粒体功能可能已经在糖尿病前期受到影响。
与代谢障碍个体(如糖尿病前期)线粒体功能下降的概念一致,在瘦人和肥胖者之间已经发现了线粒体功能的一些差异。Montaigne等人发现,在没有T2DM的肥胖个体中,体外呼吸链复合物活性异常,但这并没有导致线粒体呼吸减少[70]。这与Niemann等人一致,他们表明,与瘦人相比,肥胖者在右心房心肌细胞中的线粒体生物发生和功能(呼吸链复合体I)受到干扰[71]。此外,在临床心肌病发作之前,肥胖个体的体外收缩性能已经降低,但程度低于T2DM[70]。然而,这些结果表明,不仅在T2DM中看到的慢性高血糖症,而且在肥胖症中看到的葡萄糖稳态的早期改变,都会对线粒体功能产生影响,从而对内在的心肌收缩功能产生影响。因此,可以预料的是,肥胖个体的这些变化也存在于糖尿病前期,作为 DCM 的前奏;然而,这仍有待在新的横断面研究中探索。
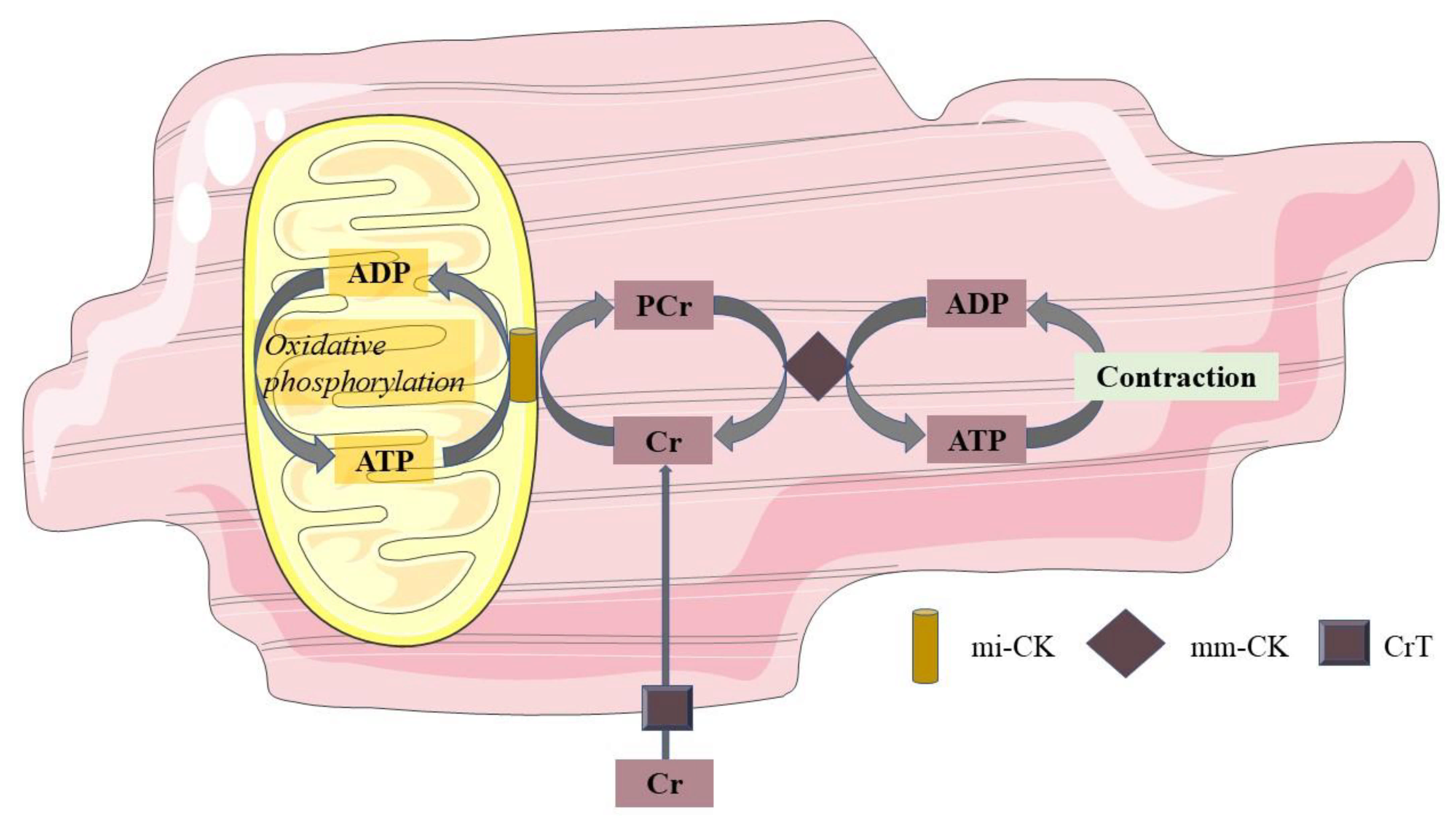
在体内,高能磷酸盐的浓度被认为与心脏线粒体氧化密切相关。这可以通过 31 P-MRS来测量。通过这种技术,可以在特定的共振频率下识别PCr和ATP。作为相对定量,PCr 与 ATP 的比率被用作心肌能量状态的衡量标准。线粒体在氧化磷酸化过程中产生 ATP,而 ATP 又可用于将肌酸 (Cr) 转化为 PCr。在肌瘤中,在能量需求增加的情况下,PCr的磷酸基团与二磷酸腺苷(ADP)交换形成ATP。通过这种方式,PCr 起到缓冲 ATP 的作用。该 PCR 穿梭系统也如图 1 所示。在正常心肌中,ATP合成可以维持在ATP需求的速率下,并且PCr水平得以维持。然而,在线粒体功能下降的心脏病中,ATP需求可能超过线粒体产生ATP的能力,因此,PCr浓度会下降[72]。因此,PCr/ATP 比率被认为是线粒体功能的标志物;然而,人们应该意识到,肌酸供应、pH和氧气供应可能独立影响心肌细胞中的PCr浓度[73]。

图 1.磷酸肌酸穿梭系统。线粒体在氧化磷酸化过程中产生 ATP,该 ATP 通过 mi-CK 将线粒体膜处的 Cr 转化为 PCr。反过来,PCr从线粒体膜穿梭到肌节,在能量需求增加的情况下,通过mm-CK,PCr的磷基团与ADP交换形成ATP。通过这种方式,PCr 起到缓冲 ATP 的作用。ADP二磷酸腺苷;ATP三磷酸腺苷;游离铬肌酐;聚氯乙烯酸磷脂酸;mi-CK线粒体肌酸激酶;mm-CK肌原纤维肌酸激酶;CrT肌酐转运蛋白。
由于离体研究提示糖尿病前期的线粒体功能下降[28,70],因此可以预期,在糖尿病前期,心肌可能不得不更多地依赖其储备(PCr)来产生ATP以满足ATP需求,导致心肌能量状态降低,如体内PCr/ATP比值所衡量的那样。尽管关于肥胖和 T2DM 中心脏线粒体功能障碍的文献正在扩大,但缺乏对糖尿病前期的研究。 31 Diamant等人和Scheuermann-Freestone等人进行的P-MRS体内研究表明,与NGM相比,T2DM的HbA1c相对较高(分别为6.1±1.1和8.3±0.4),PCr/ATP比值较低,因此与体外测量的线粒体功能降低一致[74,75]。然而,在血浆葡萄糖调节良好的T2DM个体中,Rijzewijk等人发现的PCr/ATP比值与匹配的肥胖对照组没有差异[76]。此外,Scheuermann-Freestone等人表明,T2DM和NGM患者的PCr/ATP比值与血浆FFA浓度呈负相关,而PCr/ATP与T2DM患者的血浆葡萄糖浓度呈正相关,从而表明代谢失调是心脏能量状态紊乱的标志[75],从而暗示糖尿病前期可能已经出现这种情况。
在非糖尿病患者和T2DM患者中,较低的PCr/ATP比值与舒张期心脏功能参数呈负相关,例如E加速峰、E减速峰和E峰充盈率[74]。这些人类体内MRS数据支持以下假设,即糖尿病前期状态下线粒体能量代谢的早期改变确实增加了对舒张性心力衰竭的易感性,如DCM所示。
然而,由于目前缺乏对糖尿病前期的体内研究,糖尿病前期预期的 PCr/ATP 比率降低是基于肥胖和 T2DM 数据的推测。因此,糖尿病前期线粒体功能和代谢变化的复杂病理学仍不完全清楚。正如在关于心脏脂肪的一节中已经描述的那样,潜在的机制可能涉及营养物质生物利用度过高的有害影响。这些营养素,或者更具体地说是脂肪酸,可能会影响线粒体功能。在小鼠研究中,已经表明,高丰度的脂肪酸可能导致心脏中底物氧化效率低下(反映为能量产生(ATP产生)与呼吸的比率降低),导致活性氧(ROS)的形成,从而导致线粒体损伤[67,68,77,78]。可能,类似的机制发生在糖尿病前期状态的人类心脏中。
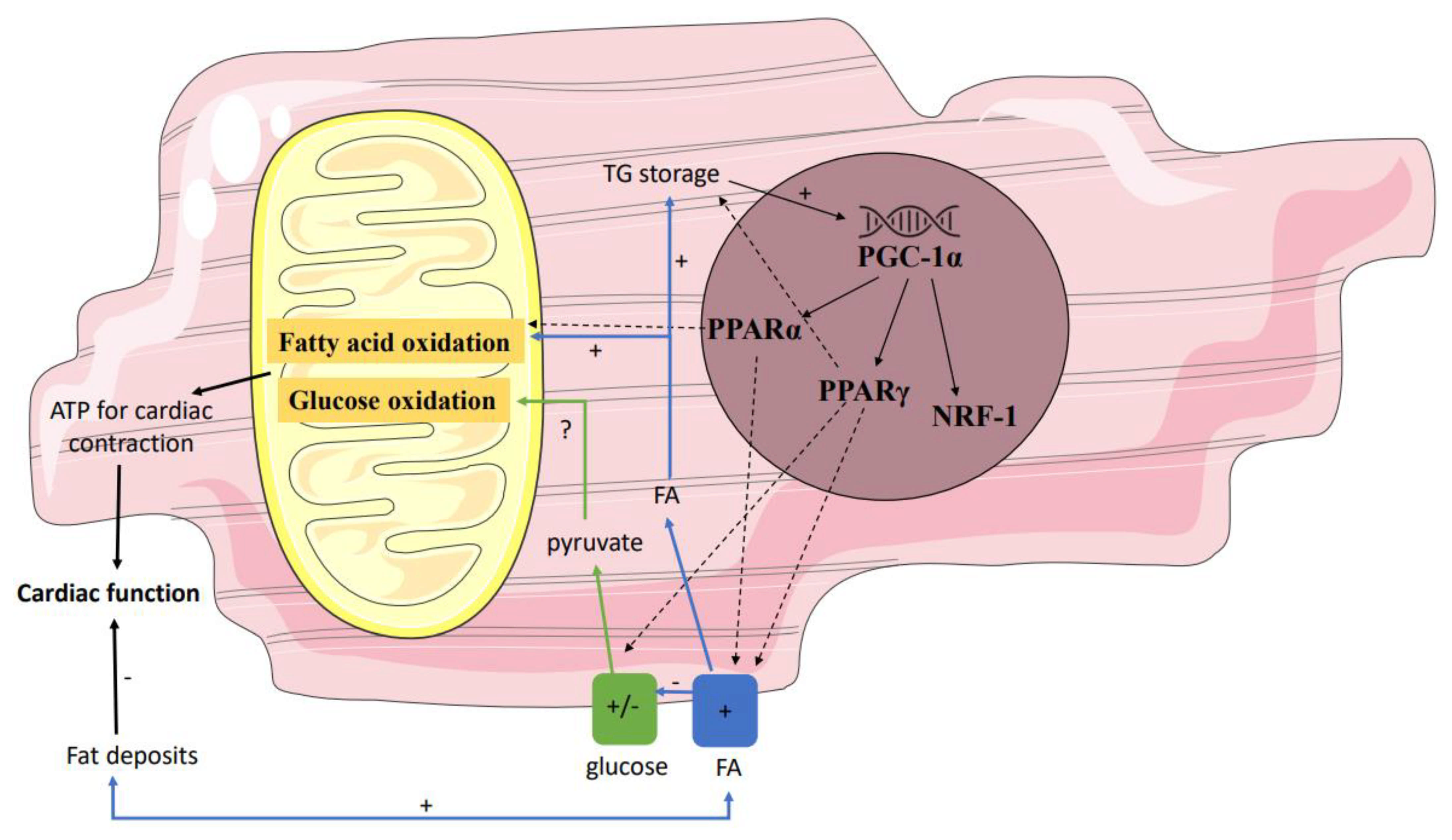
其次,基因调控途径可能通过影响各种底物的供应和氧化之间的相互作用来影响线粒体功能(图2)。不仅在T2DM患者中,而且在T2DM患者的一级亲属中,已经表明骨骼肌中过氧化物酶体增殖物激活受体(PPAR)共激活因子PGC-1α的表达降低[79]。PGC-1通常在细胞ATP需求时增加[80],导致NRF-1、PPARα和PPARγ的转录,从而可能对线粒体代谢产生间接影响。由于 NRF-1 调节许多线粒体基因(包括 OXPHOS 基因)的表达,因此 PGC-1α 的表达降低将导致 OXPHOS 复合物的线粒体含量降低。在骨骼肌中发现的这些数据可以转化为心脏,尽管缺乏糖尿病前期的数据。然而,Montaigne等人发现,在T2DM中,NRF-1和心脏线粒体功能下调[70]。

图2.影响线粒体功能的基因调控途径。几个基因影响各种底物的供应和氧化之间的相互作用。在糖尿病前期中,这些基因的下调和/或上调可能会影响线粒体功能。部分正因为如此,在糖尿病前期,脂肪酸氧化可能受到刺激,导致ATP的净减少,从而降低心肌效率。PPAR过氧化物酶体增殖物激活受体;ATP三磷酸腺苷。
除了 PGC-1α 表达降低后 NRF-1 的下调外,PPARα 和 PPARγ 也可能受到 NRF-1 的影响。已知这些PPAR受体协调脂肪酸代谢最关键调节因子的表达,因此负责确定心脏中的底物偏好。据报道,人PPARα和PPARγ基因的多态性会影响CVD的危险标志物,包括BMI、胆固醇和T2DM的发病率[81]。由于 PPAR 多态性与 T2DM 的发病率相关,因此与糖尿病前期和 T2DM 个体相比,健康个体的 PPAR 表达可能存在差异。然而,Marfella等人研究了左心室间隔的活检,发现有和没有代谢综合征的个体的心肌PPARα表达没有显著差异,尽管PPARγ在健康个体中较低[26]。此外,PPARγ的表达与LVEF和心脏脂肪的积累相关[26]。这与Anderson等人的结果一致,他们发现脂肪酸刺激后线粒体呼吸减少,但未发现T2DM心房中PGC-1α和PPARα的表达存在差异[28]。然而,这是一个相对较小的异质性患者群体。同样,一项针对 T2DM 个体的大型观察性研究(FIELD 研究)表明,使用 PPARα 激动剂(非诺贝特)并不能降低冠状动脉事件的风险;然而,它确实减少了总心血管事件,主要是由于非致死性心肌梗死和血运重建较少[82],这意味着PPARα刺激可能对T2DM有益。 这种对人类有利作用背后的机制尚不清楚,但用PPARα激动剂(GW7647)治疗在小鼠中也显示出诱导心肌缺血后对心肌收缩功能的保护作用[83],并且在不同的胰岛素抵抗动物模型中用PPARα激动剂(非诺贝特或环丙贝特)治疗(C57BL/6小鼠诱导的高脂肪饮食或肥胖Zucker大鼠遗传诱导)显示葡萄糖代谢略有改善[84]。如果动物研究的结果可以转化为人类,后者可能会解释非诺贝特在FIELD研究中的有益作用。相反,其他小鼠研究表明,脂肪酸可用性的增加导致PPARα基因调控途径的激活,从而导致糖尿病小鼠对脂肪酸的摄取增加和心功能障碍[85,86,87]。因此,PPARα激动剂对心脏功能的影响在不同的动物研究中是矛盾的,并且没有对糖尿病前期和T2DM进行干预研究。因此,事件的顺序仍不清楚,因此需要在更大的人群中进行研究,以确定PPAR基因调控途径在糖尿病前期心脏代谢异常和心功能障碍发展中的相关性。
7. Conclusions 7. 结论
糖尿病前期心脏代谢的临床研究数据很少。心肌甘油三酯含量与胰岛素敏感性相关[25],在糖尿病前期患者中升高[25,26,27,28]。虽然尚未在糖尿病前期人群中测量到心脏周围的不同脂肪沉积,但可以预期心外膜脂肪组织升高[30,37,38]。在胰岛素刺激条件下,在胰岛素刺激条件下,糖尿病前期心肌中的FFA摄取和FFA氧化均增加[45,46]。尽管T2DM患者的葡萄糖摄取和葡萄糖氧化显著降低,但少数针对糖尿病前期的研究显示结果相互矛盾,糖尿病前期的特征是否为心肌胰岛素敏感性降低仍存在问题[51,52,56,57]。线粒体功能在糖尿病前期患者中也没有得到很好的研究,但很可能不仅T2DM中的高血糖症,而且肥胖症中葡萄糖稳态的早期改变,对线粒体功能有影响,因为HbA1c与最大脂肪酸呼吸能力呈负相关[28],血浆葡萄糖浓度与PCr/ATP相关[75]。因此,可以预期,糖尿病前期的线粒体功能下降也是DCM线粒体功能障碍的前奏[67,68]。
代谢变化对糖尿病前期个体有影响,因为代谢对心脏功能的影响经常出现在不同的患者群体中。脂肪储存增加[24,26,29],心外膜脂肪组织增加[39,40,41],FFA摄取和氧化增加[46,47]以及PCr/ATP比值降低[74],对健康和代谢受损个体的心脏功能均有负面影响。尽管缺乏对糖尿病前期个体的研究,但这些结果确实支持了糖尿病前期的代谢变化可能导致舒张功能障碍的发展的观点,如DCM所示。
糖尿病前期心脏的代谢变化和相关功能障碍似乎是可逆的[44,48,65,66]。因此,在早期(糖尿病前期)状态下抵消底物代谢的这些变化并改善线粒体功能似乎很重要,因为这些变化先于 T2DM 的 DCM。这强调了干预糖尿病前期状态的研究的必要性,以便在 T2DM 和代谢综合征的发展中提供更好的心脏保护。
Author Contributions 作者贡献
V.H.W.d.W.-V.撰写了这篇论文。T.v.d.W.审阅了论文,提供了改进论文的意见,并最终批准了手稿。所有作者均已阅读并同意该手稿的出版版本。
Funding 资金
T.v.d.W.得到了荷兰糖尿病基金会的初级奖学金(资助号:2015.81.1833)的支持。
Institutional Review Board Statement
机构审查委员会声明
Informed Consent Statement
知情同意声明
Acknowledgments 确认
我们感谢荷兰心血管研究计划的支持:荷兰心脏基金会 (CVON2014-02 ENERGISE) 支持的一项计划。
Conflicts of Interest 利益冲突
作者声明他们没有利益冲突。
Abbreviations 缩写
| 1H-MRS | proton MRS 质子MRS |
| 18F-FDG | [18F]-fluorodeoxyglucose [ 18 F]-氟脱氧葡萄糖 |
| 18F-FTHA | 18F-fluoro-6-thia-heptadecanoic acid 18 F-氟-6-硫杂七烷酸 |
| 18F-FTP | 16-[18F]fluoro-4-thiapalmitate 16-[ 18 F]氟-4-噻吩酸酯 |
| A | peak late filling velocity 峰值后期填充速度 |
| ADP | adenosine diphosphate 二磷酸腺苷 |
| ATP | adenosine triphosphate 三磷酸腺苷 |
| CVD | cardiovascular disease 心血管疾病 |
| Cr 铬 | creatine 肌酸 |
| DAG | diacylglycerol 二酰基甘油 |
| DCM | diabetic cardiomyopathy 糖尿病性心肌病 |
| E | peak early filling velocity 峰值早期填充速度 |
| EAT | epicardial adipose tissue 心外膜脂肪组织 |
| FFA | free fatty acid 游离脂肪酸 |
| HSL | hormone-sensitive lipase 激素敏感脂肪酶 |
| IRS1 | insulin receptor substrate 1 胰岛素受体底物 1 |
| LVEF | left ventricular ejection fraction 左心室射血分数 |
| LVM | left ventricular mass 左心室肿块 |
| MRS | magnetic resonance spectroscopy 磁共振波谱 |
| NEFA | nonesterified fatty acid 非酯化脂肪酸 |
| NGM | normal glucose metabolism 葡萄糖代谢正常 |
| PCr 聚氯乙烯 | phosphocreatine 磷酸肌酸 |
| PET | positron emission tomography 正电子发射断层扫描 |
| PI3K | PI 3-kinases PI 3-激酶 |
| PPAR | peroxisome proliferator-activated receptor 过氧化物酶体增殖物激活受体 |
| ROS | reactive oxygen species 活性氧 |
| T2DM | type 2 diabetes mellitus 2型糖尿病 |
| TG | triglyceride 甘油三酸酯 |
References 引用
- World Health Organization; International Diabetes Federation. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation: WHO. 2006. Available online: https://www.who.int/diabetes/publications/Definition%20and%20diagnosis%20of%20diabetes_new.pdf (accessed on 12 October 2021).
世界卫生组织;国际糖尿病联合会。糖尿病和中度高血糖的定义和诊断:WHO/IDF咨询报告:WHO。2006. 可在线查阅:https://www.who.int/diabetes/publications/Definition%20and%20diagnosis%20of%20diabetes_new.pdf(2021年10月12日访问)。 - Punthakee, Z.; Goldenberg, R.; Katz, P. Definition, Classification and Diagnosis of Diabetes, Prediabetes and Metabolic Syndrome. Can. J. Diabetes 2018, 42 (Suppl. S1), S8–S11. [Google Scholar] [CrossRef] [Green Version]
- Cai, X.; Zhang, Y.; Li, M.; Wu, J.H.; Mai, L.; Li, J.; Yang, Y.; Hu, Y.; Huang, Y. Association between prediabetes and risk of all cause mortality and cardiovascular disease: Updated meta-analysis. BMJ 2020, 370, m2297. [Google Scholar] [CrossRef] [PubMed]
- Haffner, S.M.; Mykkanen, L.; Festa, A.; Burke, J.P.; Stern, M.P. Insulin-resistant prediabetic subjects have more atherogenic risk factors than insulin-sensitive prediabetic subjects: Implications for preventing coronary heart disease during the prediabetic state. Circulation 2000, 101, 975–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; Stampfer, M.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [PubMed] [Green Version]
- Grundy, S.M.; Benjamin, I.J.; Burke, G.L.; Chait, A.; Eckel, R.H.; Howard, B.V.; Mitch, W.; Smith, S.C., Jr.; Sowers, J.R. Diabetes and cardiovascular disease: A statement for healthcare professionals from the American Heart Association. Circulation 1999, 100, 1134–1146. [Google Scholar] [CrossRef] [Green Version]
- Hammoud, T.; Tanguay, J.F.; Bourassa, M.G. Management of coronary artery disease: Therapeutic options in patients with diabetes. J. Am. Coll. Cardiol. 2000, 36, 355–365. [Google Scholar] [CrossRef] [Green Version]
- Taegtmeyer, H.; McNulty, P.; Young, M.E. Adaptation and maladaptation of the heart in diabetes: Part I: General concepts. Circulation 2002, 105, 1727–1733. [Google Scholar] [CrossRef] [Green Version]
- Eckel, R.H.; York, D.A.; Rossner, S.; Hubbard, V.; Caterson, I.; St Jeor, S.T.; Hayman, L.L.; Mullis, R.M.; Blair, S.N. Prevention Conference VII: Obesity, a worldwide epidemic related to heart disease and stroke: Executive summary. Circulation 2004, 110, 2968–2975. [Google Scholar] [CrossRef]
- Calle, E.E.; Thun, M.J.; Petrelli, J.M.; Rodriguez, C.; Heath, C.W., Jr. Body-mass index and mortality in a prospective cohort of U.S. adults. N. Engl. J. Med. 1999, 341, 1097–10105. [Google Scholar] [CrossRef] [PubMed]
- Wolk, R.; Berger, P.; Lennon, R.J.; Brilakis, E.S.; Davison, D.E.; Somers, V.K. Association between plasma adiponectin levels and unstable coronary syndromes. Eur. Heart J. 2007, 28, 292–298. [Google Scholar] [CrossRef]
- Tirosh, A.; Shai, I.; Afek, A.; Dubnov-Raz, G.; Ayalon, N.; Gordon, B.; Derazne, E.; Tzur, D.; Shamis, A.; Vinker, S.; et al. Adolescent BMI trajectory and risk of diabetes versus coronary disease. N. Engl. J. Med. 2011, 364, 1315–1325. [Google Scholar] [CrossRef] [Green Version]
- Lloyd-Jones, D.; Adams, R.J.; Brown, T.M.; Carnethon, M.; Dai, S.; De Simone, G.; Ferguson, T.B.; Ford, E.; Furie, K.; Gillespie, C.; et al. Executive summary: Heart disease and stroke statistics—2010 update: A report from the American Heart Association. Circulation 2010, 121, 948–954. [Google Scholar] [PubMed]
- Van de Weijer, T.; Schrauwen-Hinderling, V.B.; Schrauwen, P. Lipotoxicity in type 2 diabetic cardiomyopathy. Cardiovasc. Res. 2011, 92, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannel, W.B.; Hjortland, M.; Castelli, W.P. Role of diabetes in congestive heart failure: The Framingham study. Am. J. Cardiol. 1974, 34, 29–34. [Google Scholar] [CrossRef]
- LeWinter, M.M.; Meyer, M. Mechanisms of diastolic dysfunction in heart failure with a preserved ejection fraction: If it’s not one thing it’s another. Circ. Heart Fail. 2013, 6, 1112–1115. [Google Scholar] [CrossRef] [Green Version]
- Markus, M.R.P.; Rospleszcz, S.; Ittermann, T.; Baumeister, S.E.; Schipf, S.; Siewert-Markus, U.; Lorbeer, R.; Storz, C.; Ptushkina, V.; Peters, A.; et al. Glucose and insulin levels are associated with arterial stiffness and concentric remodeling of the heart. Cardiovasc. Diabetol. 2019, 18, 145. [Google Scholar] [CrossRef]
- Bell, D.S. Diabetic cardiomyopathy. Diabetes Care 2003, 26, 2949–2951. [Google Scholar] [CrossRef] [Green Version]
- Bugger, H.; Abel, E.D. Molecular mechanisms of diabetic cardiomyopathy. Diabetologia 2014, 57, 660–671. [Google Scholar] [CrossRef] [Green Version]
- Atale, N.; Yadav, D.; Rani, V.; Jin, J.O. Pathophysiology, Clinical Characteristics of Diabetic Cardiomyopathy: Therapeutic Potential of Natural Polyphenols. Front. Nutr. 2020, 7, 564352. [Google Scholar] [CrossRef]
- Gulsin, G.S.; Athithan, L.; McCann, G.P. Diabetic cardiomyopathy: Prevalence, determinants and potential treatments. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819834869. [Google Scholar] [CrossRef]
- Tan, Y.; Zhang, Z.; Zheng, C.; Wintergerst, K.A.; Keller, B.B.; Cai, L. Mechanisms of diabetic cardiomyopathy and potential therapeutic strategies: Preclinical and clinical evidence. Nat. Rev. Cardiol. 2020, 17, 585–607. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.B. Abnormalities of energy expenditure and the development of obesity. Obes. Res. 1995, 3 (Suppl. S2), 155s–163s. [Google Scholar] [CrossRef]
- Szczepaniak, L.S.; Dobbins, R.L.; Metzger, G.J.; Sartoni-D’Ambrosia, G.; Arbique, D.; Vongpatanasin, W.; Unger, R.; Victor, R.G. Myocardial triglycerides and systolic function in humans: In vivo evaluation by localized proton spectroscopy and cardiac imaging. Magn. Reson. Med. 2003, 49, 417–423. [Google Scholar] [CrossRef]
- McGavock, J.M.; Lingvay, I.; Zib, I.; Tillery, T.; Salas, N.; Unger, R.; Levine, B.D.; Raskin, P.; Victor, R.G.; Szczepaniak, L.S. Cardiac steatosis in diabetes mellitus: A 1H-magnetic resonance spectroscopy study. Circulation 2007, 116, 1170–1175. [Google Scholar] [CrossRef] [Green Version]
- Marfella, R.; Di Filippo, C.; Portoghese, M.; Barbieri, M.; Ferraraccio, F.; Siniscalchi, M.; Cacciapuoti, F.; Rossi, F.; D’Amico, M.; Paolisso, G. Myocardial lipid accumulation in patients with pressure-overloaded heart and metabolic syndrome. J. Lipid Res. 2009, 50, 2314–2323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Adrogue, J.V.; Golfman, L.; Uray, I.; Lemm, J.; Youker, K.; Noon, G.P.; Frazier, O.H.; Taegtmeyer, H. Intramyocardial lipid accumulation in the failing human heart resembles the lipotoxic rat heart. FASEB J. 2004, 18, 1692–1700. [Google Scholar] [CrossRef]
- Anderson, E.J.; Kypson, A.P.; Rodriguez, E.; Anderson, C.A.; Lehr, E.J.; Neufer, P.D. Substrate-specific derangements in mitochondrial metabolism and redox balance in the atrium of the type 2 diabetic human heart. J. Am. Coll. Cardiol. 2009, 54, 1891–1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Meer, R.W.; Hammer, S.; Smit, J.W.; Frolich, M.; Bax, J.J.; Diamant, M.; de Roos, A.; Romijn, J.A.; Lamb, H.J. Short-term caloric restriction induces accumulation of myocardial triglycerides and decreases left ventricular diastolic function in healthy subjects. Diabetes 2007, 56, 2849–2853. [Google Scholar] [CrossRef] [Green Version]
- Malavazos, A.E.; Di Leo, G.; Secchi, F.; Lupo, E.N.; Dogliotti, G.; Coman, C.; Morricone, L.; Corsi, M.M.; Sardanelli, F.; Iacobellis, G. Relation of echocardiographic epicardial fat thickness and myocardial fat. Am. J. Cardiol. 2010, 105, 1831–1835. [Google Scholar] [CrossRef]
- Bakkum, M.J.; Danad, I.; Romijn, M.A.; Stuijfzand, W.J.; Leonora, R.M.; Tulevski, I.I.; Somsen, G.A.; Lammertsma, A.A.; van Kuijk, C.; van Rossum, A.C.; et al. The impact of obesity on the relationship between epicardial adipose tissue, left ventricular mass and coronary microvascular function. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1562–1573. [Google Scholar] [CrossRef] [Green Version]
- Cherian, S.; Lopaschuk, G.D.; Carvalho, E. Cellular cross-talk between epicardial adipose tissue and myocardium in relation to the pathogenesis of cardiovascular disease. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E937–E949. [Google Scholar] [CrossRef] [Green Version]
- Gaborit, B.; Abdesselam, I.; Dutour, A. Epicardial fat: More than just an “epi” phenomenon? Horm. Metab. Res. 2013, 45, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Iozzo, P. Myocardial, perivascular, and epicardial fat. Diabetes Care 2011, 34 (Suppl. S2), S371–S379. [Google Scholar] [CrossRef] [Green Version]
- Henrichot, E.; Juge-Aubry, C.E.; Pernin, A.; Pache, J.C.; Velebit, V.; Dayer, J.M.; Meda, P.; Chizzolini, C.; Meier, C.A. Production of chemokines by perivascular adipose tissue: A role in the pathogenesis of atherosclerosis? Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2594–2599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibasaki, I.; Nishikimi, T.; Mochizuki, Y.; Yamada, Y.; Yoshitatsu, M.; Inoue, Y.; Kuwata, T.; Ogawa, H.; Tsuchiya, G.; Ishimitsu, T.; et al. Greater expression of inflammatory cytokines, adrenomedullin, and natriuretic peptide receptor-C in epicardial adipose tissue in coronary artery disease. Regul. Pept. 2010, 165, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G. Local and systemic effects of the multifaceted epicardial adipose tissue depot. Nat. Rev. Endocrinol. 2015, 11, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Willens, H.J. Echocardiographic epicardial fat: A review of research and clinical applications. J. Am. Soc. Echocardiogr. 2009, 22, 1311–1319. [Google Scholar] [CrossRef]
- Dabbah, S.; Komarov, H.; Marmor, A.; Assy, N. Epicardial fat, rather than pericardial fat, is independently associated with diastolic filling in subjects without apparent heart disease. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 877–882. [Google Scholar] [CrossRef]
- Hua, N.; Chen, Z.; Phinikaridou, A.; Pham, T.; Qiao, Y.; LaValley, M.P.; Bigornia, S.J.; Ruth, M.R.; Apovian, C.M.; Ruberg, F.L.; et al. The influence of pericardial fat upon left ventricular function in obese females: Evidence of a site-specific effect. J. Cardiovasc. Magn. Reson. 2014, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Konishi, M.; Sugiyama, S.; Sugamura, K.; Nozaki, T.; Matsubara, J.; Akiyama, E.; Utsunomiya, D.; Matsuzawa, Y.; Yamashita, Y.; Kimura, K.; et al. Accumulation of pericardial fat correlates with left ventricular diastolic dysfunction in patients with normal ejection fraction. J. Cardiol. 2012, 59, 344–351. [Google Scholar] [CrossRef] [Green Version]
- Iacobellis, G.; Leonetti, F.; Singh, N.; Sharma, A.M. Relationship of epicardial adipose tissue with atrial dimensions and diastolic function in morbidly obese subjects. Int. J. Cardiol. 2007, 115, 272–273. [Google Scholar] [CrossRef]
- De Wit-Verheggen, V.H.W.; Altintas, S.; Spee, R.J.M.; Mihl, C.; van Kuijk, S.M.J.; Wildberger, J.E.; Schrauwen-Hinderling, V.B.; Kietselaer, B.; van de Weijer, T. Pericardial fat and its influence on cardiac diastolic function. Cardiovasc. Diabetol. 2020, 19, 129. [Google Scholar] [CrossRef] [PubMed]
- Hannukainen, J.C.; Lautamäki, R.; Pärkkä, J.; Strandberg, M.; Saunavaara, V.; Hurme, S.; Soinio, M.; Dadson, P.; Virtanen, K.A.; Grönroos, T.; et al. Reversibility of Myocardial Metabolism and Remodeling in Morbidly Obese Patients Six Months after Bariatric Surgery. Diabetes Obes. Metab. 2018, 20, 963–973. [Google Scholar] [CrossRef] [PubMed]
- Brassard, P.; Frisch, F.; Lavoie, F.; Cyr, D.; Bourbonnais, A.; Cunnane, S.C.; Soinio, M.; Dadson, P.; Virtanen, K.A.; Gronroos, T.; et al. Impaired plasma nonesterified fatty acid tolerance is an early defect in the natural history of type 2 diabetes. J. Clin. Endocrinol. Metab. 2008, 93, 837–844. [Google Scholar] [CrossRef]
- Labbe, S.M.; Grenier-Larouche, T.; Noll, C.; Phoenix, S.; Guerin, B.; Turcotte, E.E.; Carpentier, A.C. Increased myocardial uptake of dietary fatty acids linked to cardiac dysfunction in glucose-intolerant humans. Diabetes 2012, 61, 2701–2710. [Google Scholar] [CrossRef] [Green Version]
- Mather, K.J.; Hutchins, G.D.; Perry, K.; Territo, W.; Chisholm, R.; Acton, A.; Glick-Wilson, B.; Considine, R.V.; Moberly, S.; DeGrado, T.R. Assessment of myocardial metabolic flexibility and work efficiency in human type 2 diabetes using 16-[18F]fluoro-4-thiapalmitate, a novel PET fatty acid tracer. Am. J. Physiol. Endocrinol. Metab. 2016, 310, E452–E460. [Google Scholar] [CrossRef] [Green Version]
- Labbe, S.M.; Noll, C.; Grenier-Larouche, T.; Kunach, M.; Bouffard, L.; Phoenix, S.; Guerin, B.; Baillargeon, J.P.; Langlois, M.F.; Turcotte, E.E.; et al. Improved cardiac function and dietary fatty acid metabolism after modest weight loss in subjects with impaired glucose tolerance. Am. J. Physiol. Endocrinol. Metab. 2014, 306, E1388–E1396. [Google Scholar] [CrossRef] [PubMed]
- Noll, C.; Kunach, M.; Frisch, F.; Bouffard, L.; Dubreuil, S.; Jean-Denis, F.; Phoenix, S.; Cunnane, S.C.; Guerin, B.; Turcotte, E.E.; et al. Seven-Day Caloric and Saturated Fat Restriction Increases Myocardial Dietary Fatty Acid Partitioning in Impaired Glucose-Tolerant Subjects. Diabetes 2015, 64, 3690–3699. [Google Scholar] [CrossRef] [Green Version]
- Abel, E.D.; O’Shea, K.M.; Ramasamy, R. Insulin resistance: Metabolic mechanisms and consequences in the heart. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2068–2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.; Jo, K.; Kim, K.J.; Lee, Y.H.; Han, E.; Yoon, H.J.; Wang, H.J.; Kang, E.S.; Yun, M. Visceral adiposity is associated with altered myocardial glucose uptake measured by (18)FDG-PET in 346 subjects with normal glucose tolerance, prediabetes, and type 2 diabetes. Cardiovasc. Diabetol. 2015, 14, 148. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.; Qiu, C.; Wang, X.; Xu, M.; Shao, X.; Wang, Y. The association between diabetes mellitus and reduction in myocardial glucose uptake: A population-based 18F-FDG PET/CT study. BMC Cardiovasc. Disord. 2018, 18, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Brom, C.E.; Huisman, M.C.; Vlasblom, R.; Boontje, N.M.; Duijst, S.; Lubberink, M.; Molthoff, C.F.; Lammertsma, A.A.; van der Velden, J.; Boer, C.; et al. Altered myocardial substrate metabolism is associated with myocardial dysfunction in early diabetic cardiomyopathy in rats: Studies using positron emission tomography. Cardiovasc. Diabetol. 2009, 8, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, R.; Jorsal, A.; Iversen, P.; Tolbod, L.; Bouchelouche, K.; Sorensen, J.; Harms, H.J.; Flyvbjerg, A.; Botker, H.E.; Wiggers, H. Heart failure patients with prediabetes and newly diagnosed diabetes display abnormalities in myocardial metabolism. J. Nucl. Cardiol. 2018, 25, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Ohtake, T.; Yokoyama, I.; Watanabe, T.; Momose, T.; Serezawa, T.; Nishikawa, J.; Sasaki, Y. Myocardial glucose metabolism in noninsulin-dependent diabetes mellitus patients evaluated by FDG-PET. J. Nucl. Med. 1995, 36, 456–463. [Google Scholar] [PubMed]
- Eriksson, J.W.; Visvanathar, R.; Kullberg, J.; Strand, R.; Skrtic, S.; Ekström, S.; Lubberink, M.; Lundqvist, M.H.; Katsogiannos, P.; Pereira, M.J.; et al. Tissue-specific glucose partitioning and fat content in prediabetes and type 2 diabetes: Whole-body PET/MRI during hyperinsulinemia. Eur. J. Endocrinol. 2021, 184, 879–889. [Google Scholar] [CrossRef]
- Yokoyama, I.; Yonekura, K.; Ohtake, T.; Kawamura, H.; Matsumoto, A.; Inoue, Y.; Aoyagi, T.; Sugiura, S.; Omata, M.; Ohtomo, K.; et al. Role of insulin resistance in heart and skeletal muscle F-18 fluorodeoxyglucose uptake in patients with non-insulin-dependent diabetes mellitus. J. Nucl. Cardiol. 2000, 7, 242–248. [Google Scholar] [CrossRef]
- Cook, S.A.; Varela-Carver, A.; Mongillo, M.; Kleinert, C.; Khan, M.T.; Leccisotti, L.; Strickland, N.; Matsui, T.; Das, S.; Rosenzweig, A.; et al. Abnormal myocardial insulin signalling in type 2 diabetes and left-ventricular dysfunction. Eur. Heart J. 2010, 31, 100–111. [Google Scholar] [CrossRef] [Green Version]
- Chung, Y.H.; Lu, K.Y.; Chiu, S.C.; Lo, C.J.; Hung, L.M.; Huang, J.P.; Cheng, M.L.; Wang, C.H.; Tsai, C.K.; Lin, Y.C.; et al. Early Imaging Biomarker of Myocardial Glucose Adaptations in High-Fat-Diet-Induced Insulin Resistance Model by Using (18)F-FDG PET and [U-(13)C]glucose Nuclear Magnetic Resonance Tracer. Contrast Media Mol. Imaging 2018, 2018, 8751267. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, C.H.; Lau, J.Y.; Chen, A.P.; Geraghty, B.J.; Perks, W.J.; Roifman, I.; Wright, G.A.; Connelly, K.A. Hyperpolarized 13C Metabolic MRI of the Human Heart: Initial Experience. Circ. Res. 2016, 119, 1177–1182. [Google Scholar] [CrossRef]
- Rider, O.J.; Apps, A.; Miller, J.; Lau, J.Y.C.; Lewis, A.J.M.; Peterzan, M.A.; Dodd, M.S.; Lau, A.Z.; Trumper, C.; Gallagher, F.A.; et al. Noninvasive In Vivo Assessment of Cardiac Metabolism in the Healthy and Diabetic Human Heart Using Hyperpolarized (13)C MRI. Circ. Res. 2020, 126, 725–736. [Google Scholar] [CrossRef] [Green Version]
- Chatham, J.C.; Seymour, A.M. Cardiac carbohydrate metabolism in Zucker diabetic fatty rats. Cardiovasc. Res. 2002, 55, 104–112. [Google Scholar] [CrossRef]
- Chatham, J.C.; Forder, J.R. A 13C-NMR study of glucose oxidation in the intact functioning rat heart following diabetes-induced cardiomyopathy. J. Mol. Cell. Cardiol. 1993, 25, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Le Page, L.M.; Rider, O.J.; Lewis, A.J.; Ball, V.; Clarke, K.; Johansson, E.; Carr, C.A.; Heather, L.C.; Tyler, D.J. Increasing Pyruvate Dehydrogenase Flux as a Treatment for Diabetic Cardiomyopathy: A Combined 13C Hyperpolarized Magnetic Resonance and Echocardiography Study. Diabetes 2015, 64, 2735–2743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morbelli, S.; Marini, C.; Adami, G.F.; Kudomi, N.; Camerini, G.; Iozzo, P.; Massollo, M.; Capitanio, S.; Bodrato, S.; Verardi, M.T.; et al. Tissue specificity in fasting glucose utilization in slightly obese diabetic patients submitted to bariatric surgery. Obesity 2013, 21, E175–E181. [Google Scholar] [CrossRef] [Green Version]
- Lautamäki, R.; Airaksinen, K.E.J.; Seppänen, M.; Toikka, J.; Luotolahti, M.; Ball, E.; Borra, R.; Härkönen, R.; Iozzo, P.; Stewart, M.; et al. Rosiglitazone Improves Myocardial Glucose Uptake in Patients with Type 2 Diabetes and Coronary Artery Disease. A 16-Week Randomized, Double-Blind, Placebo-Controlled Study. Diabetes 2005, 54, 2787–2794. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.A.; Wei, Y.; Sowers, J.R. Role of mitochondrial dysfunction in insulin resistance. Circ. Res. 2008, 102, 401–414. [Google Scholar] [CrossRef]
- Jia, G.; DeMarco, V.G.; Sowers, J.R. Insulin resistance and hyperinsulinaemia in diabetic cardiomyopathy. Nat. Rev. Endocrinol. 2016, 12, 144–153. [Google Scholar] [CrossRef]
- Koncsos, G.; Varga, Z.V.; Baranyai, T.; Boengler, K.; Rohrbach, S.; Li, L.; Borra, R.; Härkönen, R.; Iozzo, P.; Stewart, M.; et al. Diastolic dysfunction in prediabetic male rats: Role of mitochondrial oxidative stress. Am. J. Physiol. Heart Circ. Physiol. 2016, 311, H927–H943. [Google Scholar] [CrossRef] [Green Version]
- Montaigne, D.; Marechal, X.; Coisne, A.; Debry, N.; Modine, T.; Fayad, G.; Potelle, C.; El Arid, J.M.; Mouton, S.; Sebti, Y.; et al. Myocardial contractile dysfunction is associated with impaired mitochondrial function and dynamics in type 2 diabetic but not in obese patients. Circulation 2014, 130, 554–564. [Google Scholar] [CrossRef] [Green Version]
- Niemann, B.; Chen, Y.; Teschner, M.; Li, L.; Silber, R.E.; Rohrbach, S. Obesity induces signs of premature cardiac aging in younger patients: The role of mitochondria. J. Am. Coll. Cardiol. 2011, 57, 577–585. [Google Scholar] [CrossRef] [Green Version]
- Van de Weijer, T.; Paiman, E.H.M.; Lamb, H.J. Mini-Review on Cardiac Metabolic Imaging: Current imaging modalities and future perspectives. J. Appl. Physiol. 2018, 124, 168–181. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.; Jenkins, D. Factors affecting the rate of phosphocreatine resynthesis following intense exercise. Sports Med. 2002, 32, 761–784. [Google Scholar] [CrossRef] [PubMed]
- Diamant, M.; Lamb, H.J.; Groeneveld, Y.; Endert, E.L.; Smit, J.W.; Bax, J.J.; Romijn, J.A.; de Roos, A.; Radder, J.K. Diastolic dysfunction is associated with altered myocardial metabolism in asymptomatic normotensive patients with well-controlled type 2 diabetes mellitus. J. Am. Coll. Cardiol. 2003, 42, 328–335. [Google Scholar] [CrossRef] [Green Version]
- Scheuermann-Freestone, M.; Madsen, P.L.; Manners, D.; Blamire, A.M.; Buckingham, R.E.; Styles, P.; Radda, G.K.; Neubauer, S.; Clarke, K. Abnormal cardiac and skeletal muscle energy metabolism in patients with type 2 diabetes. Circulation 2003, 107, 3040–3046. [Google Scholar] [CrossRef]
- Rijzewijk, L.J.; van der Meer, R.W.; Lamb, H.J.; de Jong, H.W.; Lubberink, M.; Romijn, J.A.; Bax, J.J.; de Roos, A.; Twisk, J.W.; Heine, R.J.; et al. Altered myocardial substrate metabolism and decreased diastolic function in nonischemic human diabetic cardiomyopathy: Studies with cardiac positron emission tomography and magnetic resonance imaging. J. Am. Coll. Cardiol. 2009, 54, 1524–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, G.; Hill, M.A.; Sowers, J.R. Diabetic Cardiomyopathy: An Update of Mechanisms Contributing to This Clinical Entity. Circ. Res. 2018, 122, 624–638. [Google Scholar] [CrossRef] [PubMed]
- Aon, M.A.; Tocchetti, C.G.; Bhatt, N.; Paolocci, N.; Cortassa, S. Protective mechanisms of mitochondria and heart function in diabetes. Antioxid. Redox Signal. 2015, 22, 1563–1586. [Google Scholar] [CrossRef] [Green Version]
- Patti, M.E.; Butte, A.J.; Crunkhorn, S.; Cusi, K.; Berria, R.; Kashyap, S.; Miyazaki, Y.; Kohane, I.; Costello, M.; Saccone, R.; et al. Coordinated reduction of genes of oxidative metabolism in humans with insulin resistance and diabetes: Potential role of PGC1 and NRF1. Proc. Natl. Acad. Sci. USA 2003, 100, 8466–8471. [Google Scholar] [CrossRef] [Green Version]
- Lehman, J.J.; Barger, P.M.; Kovacs, A.; Saffitz, J.E.; Medeiros, D.M.; Kelly, D.P. Peroxisome proliferator-activated receptor gamma coactivator-1 promotes cardiac mitochondrial biogenesis. J. Clin. Investig. 2000, 106, 847–856. [Google Scholar] [CrossRef] [Green Version]
- Gilde, A.; Fruchart, J.C.; Staels, B. PPAR receptors at the crossroads of obesity, diabetes and cardiovascular diseases. Journ. Annu. Diabetol. Hotel Dieu 2007, 21–38. [Google Scholar]
- Keech, A.; Simes, R.J.; Barter, P.; Best, J.; Scott, R.; Taskinen, M.R.; Forder, P.; Pillai, A.; Davis, T.; Glasziou, P.; et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): Randomised controlled trial. Lancet 2005, 366, 1849–1861. [Google Scholar] [CrossRef]
- Yue, T.L.; Bao, W.; Jucker, B.M.; Gu, J.L.; Romanic, A.M.; Brown, P.J.; Cui, J.; Thudium, D.T.; Boyce, R.; Burns-Kurtis, C.L.; et al. Activation of peroxisome proliferator-activated receptor-alpha protects the heart from ischemia/reperfusion injury. Circulation 2003, 108, 2393–2399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerre-Millo, M.; Gervois, P.; Raspé, E.; Madsen, L.; Poulain, P.; Derudas, B.; Herbert, J.M.; Winegar, D.A.; Willson, T.M.; Fruchart, J.C.; et al. Peroxisome proliferator-activated receptor alpha activators improve insulin sensitivity and reduce adiposity. J. Biol. Chem. 2000, 275, 16638–16642. [Google Scholar] [CrossRef] [Green Version]
- Finck, B.N.; Han, X.; Courtois, M.; Aimond, F.; Nerbonne, J.M.; Kovacs, A.; Gross, R.W.; Kelly, D.P. A critical role for PPARalpha-mediated lipotoxicity in the pathogenesis of diabetic cardiomyopathy: Modulation by dietary fat content. Proc. Natl. Acad. Sci. USA 2003, 100, 1226–1231. [Google Scholar] [CrossRef] [Green Version]
- Finck, B.N.; Lehman, J.J.; Leone, T.C.; Welch, M.J.; Bennett, M.J.; Kovacs, A.; Han, X.; Gross, R.W.; Kozak, R.; Lopaschuk, G.D.; et al. The cardiac phenotype induced by PPARalpha overexpression mimics that caused by diabetes mellitus. J. Clin. Investig. 2002, 109, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Sambandam, N.; Morabito, D.; Wagg, C.; Finck, B.N.; Kelly, D.P.; Lopaschuk, G.D. Chronic activation of PPARalpha is detrimental to cardiac recovery after ischemia. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H87–H95. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Wit-Verheggen, V.H.W.; van de Weijer, T. Changes in Cardiac Metabolism in Prediabetes. Biomolecules 2021, 11, 1680. https://doi.org/10.3390/biom11111680
de Wit-Verheggen VHW, van de Weijer T. Changes in Cardiac Metabolism in Prediabetes. Biomolecules. 2021; 11(11):1680. https://doi.org/10.3390/biom11111680
Chicago/Turabian Stylede Wit-Verheggen, Vera H. W., and Tineke van de Weijer. 2021. "Changes in Cardiac Metabolism in Prediabetes" Biomolecules 11, no. 11: 1680. https://doi.org/10.3390/biom11111680

{kind=link}
{kind=link}