IMHA: Diagnosing and treating a complex disease
IMHA:診斷與治療一種複雜疾病
A careful diagnostic process will help you determine whether your veterinary patients will require long-term immunosuppressive therapy.
謹慎的診斷流程將幫助您判斷獸醫病患是否需要長期免疫抑制治療
Autoimmune hemolytic anemia, or immune-mediated hemolytic anemia (IMHA), is a complex disease in which hemolysis occurs because of antierythrocyte antibody production. This article explores the pathophysiology of primary and secondary IMHA and diagnostic and treatment options, as well as prognosis in dogs and cats.
自體免疫性溶血性貧血,或稱免疫媒介性溶血性貧血(IMHA),是一種因抗紅血球抗體產生而導致溶血發生的複雜疾病。本文探討原發性與繼發性 IMHA 的病理生理學、診斷與治療選項,以及犬貓的預後情況。
Our review of the recent literature regarding IMHA in veterinary patients reveals a focus on individual cases and a lack of controlled clinical studies, which makes a detailed review of IMHA triggers and treatment options difficult.
我們回顧近期關於獸醫患者 IMHA 的文獻發現,研究多聚焦於個別案例且缺乏對照臨床試驗,這使得對 IMHA 誘發因素與治療選項的詳細評估變得困難。


Kip Carter 基普·卡特
HEMOLYTIC ANEMIA VS. IMHA
溶血性貧血 vs. IMHA
Many causes of anemia exist in dogs and cats, so a clear distinction should be drawn between hemolytic anemia and IMHA.
犬貓貧血的原因眾多,因此必須明確區分溶血性貧血與免疫介導性溶血性貧血(IMHA)。
Hemolytic anemia 溶血性貧血
Hemolytic anemias are conditions in which red blood cells (RBCs) are destroyed at an accelerated rate and a normal regenerative response is seen in the bone marrow.
溶血性貧血是指紅血球(RBCs)加速破壞,同時骨髓出現正常再生反應的病症。
In these non-immune-mediated conditions, RBCs can be destroyed as a result of inherited membrane and enzyme defects, increased fragility from oxidative damage, or metabolic causes such as hypophosphatemia or water intoxication.1 Traditional immune-mediated mechanisms (immunoglobulins, complement) do not mediate lysis in hemolytic anemia.
在這些非免疫介導的病症中,紅血球可能因遺傳性細胞膜與酵素缺陷、氧化損傷導致的脆弱性增加,或低磷血症、水中毒等代謝性原因而遭到破壞。傳統的免疫介導機制(免疫球蛋白、補體)並不會在溶血性貧血中引發溶血作用。
Instead, destruction occurs because of factors such as increased osmotic fragility, decreased RBC function in an alkalemic environment, or increased clearance from oxidative damage.1 Unlike the treatment of immune-mediated anemia, immunosuppression is generally not used to treat hemolytic anemias.
相反,紅血球的破壞是由於滲透脆性增加、鹼性環境中紅血球功能降低或氧化損傷導致清除率增加等因素所致。1 與治療免疫介導性貧血不同,免疫抑制療法通常不用於治療溶血性貧血。
Thus, it is imperative to investigate whether an anemia has an underlying cause before assuming it is immune-mediated.
因此,在假設貧血為免疫介導性之前,必須先調查是否存在潛在病因。
Below we discuss some of the common causes of hemolytic anemia. A more exhaustive list can be found in Table 1.
以下我們將討論一些常見的溶血性貧血原因。更詳盡的清單可參見表 1。


Table 1: Selected Causes of Canine and Feline Non-immune-mediated Hemolytic Anemia
表 1:犬貓非免疫介導性溶血性貧血的部分病因
Zinc and copper toxicosis. One of the most common causes of hemolytic anemia in dogs is zinc toxicosis from the ingestion of zinc-containing objects. High zinc concentrations can be found in pennies minted since 1983, board game pieces, zippers, zinc oxide ointment, and various other sources.
鋅與銅中毒。犬隻溶血性貧血最常見的病因之一,是攝入含鋅物體導致的鋅中毒。1983 年後鑄造的硬幣、桌遊配件、拉鍊、氧化鋅軟膏及其他多種來源都可能含有高濃度鋅。
Zinc toxicosis can cause a severe intravascular hemolysis that is associated with small amounts of Heinz body and spherocyte formation. Hemolysis from zinc toxicosis can be easily mistaken for IMHA if a survey abdominal radiographic examination is not performed. Treatment consists of removing the foreign object and providing supportive care.
鋅中毒可能引發嚴重的血管內溶血,並伴隨少量海因茲小體及球形紅血球形成。若未進行腹部 X 光檢查,鋅中毒導致的溶血現象極易被誤診為免疫媒介性溶血性貧血(IMHA)。治療方式包括移除異物及提供支持性照護。
Copper toxicosis can also result in a marked intravascular hemolysis and methemoglobinemia.1
銅中毒同樣可能導致顯著的血管內溶血及變性血紅素血症。1
Heinz body anemia. Heinz bodies are dark-staining refractile material that indicate irreversibly denatured and precipitated hemoglobin in RBCs and can occur from oxidative damage in animals that have ingested onions or received drugs such as methylene blue, dl-methionine, or vitamin K3.1 In some cases of hemolytic anemia, eccentrocytes—cells in which the damaged hemoglobin is clustered together and shifted to one side of the RBC membrane, leaving a clear crescent-shaped region—are also present.
海因茲小體貧血。海因茲小體是一種深染的折光物質,代表紅血球中不可逆變性且沉澱的血紅蛋白,可能因動物攝入洋蔥或接受如亞甲藍、dl-蛋氨酸或維生素 K3 等藥物而發生氧化損傷所致。在某些溶血性貧血病例中,還可觀察到偏心球——這種紅血球的受損血紅蛋白聚集並偏向細胞膜一側,留下清晰新月形區域的異常細胞。
Eccentrocytes and cells containing Heinz bodies have less deformability and more rigidity, making them more likely to be lysed or removed from the circulation by the spleen.
含有海因茲小體及偏心球的紅血球可變形性降低且更為僵硬,因此更容易發生溶血或被脾臟從循環中清除。
Feline RBCs are especially sensitive to oxidative damage because of a high number of sulfhydryl groups in their hemogloblin. In addition, feline spleens, because of their nonsinusal conformation, are less effective at removing Heinz bodies than are canine sinusal spleens.
貓科動物的紅血球對氧化損傷特別敏感,因其血紅蛋白中含有大量巰基。此外,由於貓脾臟非竇狀結構的特性,其清除海因茲小體的效率低於犬類的竇狀脾臟。
Thus, Heinz body anemia is more commonly seen in cats and can be present during toxicosis as well as in a variety of other diseases such as hyperthyroidism, diabetes mellitus, and lymphoma.1
因此,海因茲小體貧血在貓科動物中更為常見,不僅可能出現在中毒情況,也可能伴發於多種疾病如甲狀腺功能亢進、糖尿病及淋巴瘤等。
Hypophosphatemia. Hypophosphatemia can also cause hemolytic anemia in patients being treated for diabetes mellitus, hepatic lipidosis, starvation, and other conditions.1 In these cases, it is thought that an abrupt drop in plasma phosphate concentrations can cause a concurrent depletion of RBC adenosine triphosphate, diphosphoglycerate, and reduced glutathione.
低磷血症。低磷血症也可能導致正在接受糖尿病、肝性脂肪沉積症、飢餓及其他病症治療的患者出現溶血性貧血。1 在這些案例中,被認為是血漿磷酸鹽濃度突然下降,可能同時導致紅血球內三磷酸腺苷、二磷酸甘油酸及還原型穀胱甘肽的耗竭。
These depletions lead to less deformability, more osmotic fragility, and more susceptibility to oxidative injury in erythrocytes. A rapid drop in packed cell volume and a mild Heinz body anemia can be seen in animals with hypophosphatemia. Treatment consists of phosphate supplementation (intravenous in cases of severe depletion, oral in mild cases).1
這些物質的耗竭會導致紅血球變形能力降低、滲透脆性增加,以及對氧化損傷的敏感性提高。在患有低磷血症的動物身上,可觀察到血容比快速下降及輕度的海因茲小體性貧血。治療方式包括補充磷酸鹽(嚴重缺乏時靜脈注射,輕微時口服)。1
Primary and secondary IMHA
原發性與繼發性免疫媒介性溶血性貧血
IMHA has been described in people, dogs, cats, and a wide range of other species.2 In dogs, it is estimated that 60% to 75% of cases are considered primary (idiopathic), meaning that no underlying cause can be found.3 It is thought that as more intense clinical investigations are conducted in these patients, underlying diseases and triggers will be discovered.3 Any breed can be affected with primary IMHA, but certain breeds—such as cocker spaniels, poodles, Irish setters, and Old English sheepdogs—seem to be overrepresented (Table 2).1 In both people and dogs, there appears to be a linkage between specific human leukocyte antigen (HLA) and dog leukocyte antigen (DLA) haplotypes and autoimmune disease, although the genes involved may differ for each disease. A recent study in dogs investigated whether a genetic mutation in the DLA of certain breeds predisposes them to IMHA.
免疫介導性溶血性貧血(IMHA)在人類、犬隻、貓咪及多種其他物種中均有文獻記載。2 在犬隻病例中,估計有 60%至 75%屬於原發性(特發性),意味著找不到潛在病因。3 隨著對這些病患進行更深入的臨床檢查,預期將能發現潛在疾病與誘發因子。3 任何品種都可能罹患原發性 IMHA,但某些品種如可卡犬、貴賓犬、愛爾蘭雪達犬和古代英國牧羊犬的發病率似乎偏高(表 2)。1 無論是人類或犬隻,特定的人類白血球抗原(HLA)與犬類白血球抗原(DLA)單倍型似乎都與自體免疫疾病有關聯,儘管每種疾病涉及的基因可能不同。近期一項針對犬隻的研究探討了某些品種的 DLA 基因突變是否會增加罹患 IMHA 的風險。
The results suggest that more than one gene may be involved in these susceptible breeds.4
研究結果顯示,這些易感品種可能涉及多個基因的影響。4



Table 2: Selected Causes of Canine and Feline IMHA
表 2:犬貓 IMHA 的常見病因
In secondary IMHA, RBC destruction occurs as a consequence of the immune system reacting to some condition or being activated by an agent. The end result is that the RBCs are destroyed as innocent bystanders. The process is probably the result of several factors, including an animal's susceptibility to disease and its propensity to form an autoimmune response.
在續發性免疫媒介溶血性貧血(IMHA)中,紅血球(RBC)的破壞是免疫系統對某種狀況產生反應或受到某種因子激活所導致的結果。最終導致紅血球成為無辜的旁觀者而被破壞。這個過程可能是多種因素共同作用的結果,包括動物對疾病的易感性及其形成自體免疫反應的傾向。
Usually, the process results from a combination of environmental factors and a genetic predisposition.
通常,這個過程是環境因素與遺傳易感性共同作用的結果。
The cellular mechanisms by which an agent can cause autoimmunity can include infection of immune cells, activation of lymphocytes from exposure to cytokines, cross-reactivity between microorganisms and host tissues, and the production of drug-specific antibodies with the formation of immune complexes.2 The loss of self-tolerance, resulting in autoimmunity, is also a mechanism by which hemolytic anemia can occur.
導致自體免疫的細胞機制可能包括:免疫細胞感染、暴露於細胞激素引起的淋巴細胞活化、微生物與宿主組織之間的交叉反應,以及藥物特異性抗體的產生與免疫複合物的形成。2 自我耐受性的喪失導致自體免疫,也是可能引發溶血性貧血的機制之一。
A recent report linked the class III antiarrhythmic agent amiodarone with a positive Coombs test result in two dogs.
最近一份報告指出,第三類抗心律不整藥物胺碘酮(amiodarone)與兩隻犬隻的庫姆斯試驗(Coombs test)陽性結果有關聯。
One of these patients developed hemolytic anemia, the other developed thrombocytopenia.5 Another report discussed intravascular hemolysis associated with a patent ductus arteriosus coil embolization in a dog.6 Examples of possible underlying conditions causing secondary IMHA are listed in Table 2 and include infections, drugs, and neoplasia, as well as other immune-related disorders. Secondary IMHA is the common type of immune-mediated hemolysis in cats.1
其中一名患者出現溶血性貧血,另一名則發生血小板減少症。5 另一份報告討論了犬隻因動脈導管未閉線圈栓塞術導致的血管內溶血案例。6 表 2 列出了可能導致續發性免疫媒介溶血性貧血(IMHA)的潛在病因,包括感染、藥物、腫瘤以及其他免疫相關疾病。續發性 IMHA 是貓咪最常見的免疫媒介溶血類型。1
In certain infectious diseases, such as mycoplasmosis and babesiosis, hemolysis caused by the organism is exacerbated by the body's own immune response. If you suspect an infectious disease, administer antibiotics pending the results of antibody titers or polymerase chain reaction (PCR) testing.
在某些傳染性疾病中,例如黴漿菌症和巴貝斯蟲病,病原體引起的溶血會因機體自身免疫反應而加劇。若懷疑傳染性疾病,應在抗體效價或聚合酶鏈反應(PCR)檢測結果出來前先投予抗生素。
Additionally, to reduce the body's response to the infectious agent, immunosuppressive medications often need to be administered. Once an underlying infectious agent is identified, the immunosuppressive medications can be used at lower doses and for an abridged treatment course.
此外,為降低機體對病原體的反應,通常需要給予免疫抑制藥物。一旦確認潛在病原體,便可降低免疫抑制藥物的劑量並縮短療程。
PATHOPHYSIOLOGY 病理生理學
IMHA is a type II hypersensitivity reaction in which RBCs are destroyed by the body's own immune system. The process typically involves a breakdown of immune self-tolerance and the production of anti-erythrocyte antibodies, IgG, or IgM.
免疫介導性溶血性貧血(IMHA)屬於第二型過敏反應,紅血球(RBCs)會被自身免疫系統破壞。此過程通常涉及免疫自我耐受性的崩解,以及抗紅血球抗體、IgG 或 IgM 的產生。
These antibodies are often recognizing and reacting to RBC membrane glycoproteins.7 Erythrocyte destruction is initiated when the surface becomes coated with complement and either IgM or IgG.8
這些抗體通常會識別並與紅血球膜上的醣蛋白發生反應。7 當紅血球表面被補體和 IgM 或 IgG 包覆時,便會啟動紅血球的破壞過程。8
The most common form of IMHA is IgG-mediated. The IgG-coated RBCs are destroyed by macrophages located in the liver or spleen (extravascular). Macrophages either consume the entire erythrocyte or remove a portion of the membrane, leaving smaller RBCs with no central pallor (spherocytes). These rigid spherocytes are then trapped in the spleen and destroyed.
最常見的 IMHA 形式是由 IgG 介導的。被 IgG 包覆的紅血球會被位於肝臟或脾臟(血管外)的巨噬細胞破壞。巨噬細胞會吞噬整個紅血球或移除部分細胞膜,留下沒有中央蒼白區的較小紅血球(球形紅血球)。這些僵硬的球形紅血球隨後會在脾臟中被捕捉並破壞。
IgM-coated RBCs will also activate complement more efficiently than IgG, with destruction generally occurring within vessels (intravascular).1
被 IgM 包覆的紅血球也比 IgG 更能有效激活補體,其破壞通常發生在血管內。1
SIGNALMENT, HISTORY, AND CLINICAL SIGNS IN DOGS
犬隻的品種、病史與臨床症狀
The age of onset of IMHA in a patient varies; however, the disease frequently occurs in young to middle-aged dogs. Females may be predisposed to developing IMHA.
免疫介導性溶血性貧血(IMHA)的發病年齡不一,但常見於年輕至中年犬隻。雌性犬可能較易罹患此病。


Rules of thumb for diagnosing and treating IMHA in dogs and cats
犬貓 IMHA 診斷與治療的基本原則
Patients can have an acute or a chronic history of malaise. Vomiting or diarrhea may occur before the classic signs of anemia, which are lethargy, inappetence, polyuria, polydipsia, pallor, tachypnea, and changes in urine color. Clinical signs can include weakness, pale or icteric mucous membranes, bounding pulses, tachypnea, tachycardia, hepatosplenomegaly, or a heart murmur.
病患可能出現急性或慢性的不適病史。在典型貧血症狀(如嗜睡、食慾不振、多尿、煩渴、蒼白、呼吸急促及尿液變色)出現前,可能先發生嘔吐或腹瀉。臨床症狀可包括虛弱、黏膜蒼白或黃疸、洪脈、呼吸急促、心搏過速、肝脾腫大或心雜音。
A patient's clinical signs may be related to an underlying disease process rather than the anemia itself.1
患者的臨床症狀可能與潛在疾病過程有關,而非貧血本身。1
To investigate potential underlying causes of IMHA, obtain a thorough and specific history. Ask questions regarding a wide range of environmental and historical circumstances to determine the following:
為調查 IMHA 的潛在病因,需獲取完整且詳細的病史。詢問涵蓋廣泛環境與歷史情況的問題以確定以下事項:
1. Propensity to ingest foreign objects
1. 攝入異物的傾向
2. Diet and treat history (e.g. recent ingestion of onions or garlic)
2. 飲食與零食歷史(例如近期是否攝入洋蔥或大蒜)
3. Recent history of vaccine or drug administration
3. 近期疫苗或藥物接種史
4. Travel history 4. 旅遊史
5. History of transfusions or recent dog fights
5. 輸血史或近期犬隻打鬥
6. Recent tick exposure or bee stings
6. 近期蜱蟲接觸或蜜蜂叮咬史
7. Heartworm preventive status
7. 心絲蟲預防狀態
8. Reproductive status 8. 生殖狀態
9. Signs related to other underlying disease, such as hematemesis (zinc-containing foreign body), vaginal discharge (pyometra), or weight loss and malaise (neoplasia).
9. 與其他潛在疾病相關的徵兆,例如嘔血(含鋅異物)、陰道分泌物(子宮蓄膿)或體重減輕與不適(腫瘤)。
DIAGNOSTIC TESTS IN DOGS 犬隻診斷檢測
Baseline tests recommended for diagnosing IMHA and investigating causes of secondary IMHA include a complete blood count, a reticulocyte count, a serum chemistry profile, a blood smear, a slide agglutination test, a direct Coombs test, and abdominal and thoracic radiography.
診斷免疫媒介性溶血性貧血(IMHA)及調查繼發性 IMHA 病因的基礎檢測項目包括:全血球計數、網織紅血球計數、血清生化檢查、血液抹片檢查、玻片凝集試驗、直接庫姆斯試驗,以及腹部與胸腔 X 光攝影。
Complete blood count 全血球計數
Complete blood count abnormalities usually include a regenerative anemia, although as many as 33% to 50% of dogs with IMHA can have nonregenerative anemia because of an immune attack at the level of the bone marrow or early disease.9,10 A mild to marked increase in the white blood cell count can be seen, occasionally with a left shift and toxic neutrophils.
全血球計數異常通常會出現再生性貧血,但仍有 33%至 50%的 IMHA 犬隻可能因骨髓層面的免疫攻擊或疾病早期階段而呈現非再生性貧血[9,10]。可觀察到輕度至顯著的白血球增多現象,偶伴隨核左移及中毒性中性球。
This leukocytosis can be a result of many factors, including glucocorticoid-induced leukocytosis, anemic hypoxia, thromboembolic disease, and tissue necrosis.11 A patient presenting with concurrent severe thrombocytopenia (< 50,000 platelets/µl) can have clinical signs such as petechiation, ecchymosis, epistaxis, or melena.
此白血球增多可能由多種因素引起,包括糖皮質激素誘發的白血球增多、貧血性缺氧、血栓栓塞性疾病及組織壞死[11]。若患者同時出現嚴重血小板減少症(<50,000 血小板/µl),可能出現瘀點、瘀斑、鼻出血或黑便等臨床症狀。
Low platelet counts have been associated with a greater risk of thromboembolism and a higher mortality rate in dogs.12
血小板計數偏低與犬隻發生血栓栓塞的風險增加及死亡率升高有關。12
Serum chemistry profile 血清生化檢查
Serum chemistry profile abnormalities may reflect organ damage from hypoxia while also indicating an underlying disease process.
血清生化檢查異常可能反映缺氧導致的器官損傷,同時也顯示潛在的疾病進程。
Elevated liver enzyme activities (alkaline phosphatase, alanine transaminase, and aspartate transaminase) and serum bilirubin concentrations are common.13 Even before glucocorticoid administration, many patients can have elevated liver enzyme activities from hepatic hypoxia, inflammation, or necrosis.13 Bilirubin concentrations can also be normal if the hemolysis has been chronic and the liver has had time to metabolize the bilirubin.1 Some studies have found a correlation between elevated bilirubin concentrations and increased mortality, while others have not.12-14 Other serum chemistry abnormalities may reflect underlying conditions.
常見的異常包括肝臟酵素活性升高(鹼性磷酸酶、丙氨酸轉氨酶和天門冬氨酸轉氨酶)以及血清膽紅素濃度上升。13 即使在給予糖皮質激素治療前,許多病患可能因肝臟缺氧、發炎或壞死而出現肝臟酵素活性升高的現象。13 若溶血為慢性病程且肝臟已有時間代謝膽紅素,膽紅素濃度也可能維持正常值。1 部分研究發現膽紅素濃度升高與死亡率增加具有相關性,但其他研究則未發現此關聯。12-14 其他血清生化異常可能反映潛在的疾病狀況。
A recent study concluded that an increased blood urea nitrogen concentration and band neutrophils, a decrease in platelets, and petechiation at the time of diagnosis were all negative prognostic indicators in dogs presenting with primary IMHA.3 Anecdotally, the presence of intravascular hemolysis also appears to impart a poorer prognosis in these patients.
最近一項研究得出結論,在患有原發性免疫介導性溶血性貧血(IMHA)的犬隻中,診斷時出現血尿素氮濃度升高、帶狀中性粒細胞增多、血小板減少以及瘀斑等症狀,均為不良預後指標。3 根據臨床觀察,這些病患若同時存在血管內溶血現象,預後似乎更差。
Macroagglutination and blood smear evaluations
巨凝集反應與血液抹片評估
Preparing two blood slides is imperative in diagnosing IMHA and should be performed at the outset in every suspected case. On the first slide, mix a drop of blood with a drop of saline solution, gently agitate the mixture, and then visually inspect it for macroagglutination.
診斷 IMHA 時必須製備兩張血液抹片,且應在所有疑似病例初期就進行此項檢查。在第一張玻片上,將一滴血液與一滴生理鹽水混合,輕輕搖晃混合液後,目視檢查是否出現巨凝集反應。
On the second slide, you can evaluate a blood smear in-house and also send it to a clinical pathologist for evaluation of spherocytes (Figure 1), Heinz bodies, blood parasites, and microagglutination (Figure 2). Spherocytes and erythrocyte macroagglutination and microagglutination are commonly found on blood smears in patients with IMHA. As many as 89% of dogs with IMHA have spherocytes; however, dogs with secondary hemolysis from hypophosphatemia, zinc intoxication, or splenic disease can also have them in small numbers.1,14
在第二張投影片上,您可以在院內評估血液抹片,同時也可將其送交臨床病理學家進行評估,包括球形紅血球(圖 1)、海因茲小體、血液寄生蟲以及微凝集現象(圖 2)。在 IMHA 患者的血液抹片中,通常可發現球形紅血球及紅血球的巨凝集與微凝集現象。高達 89%罹患 IMHA 的犬隻會出現球形紅血球;然而,因低磷血症、鋅中毒或脾臟疾病引發繼發性溶血犬隻也可能出現少量球形紅血球。1,14


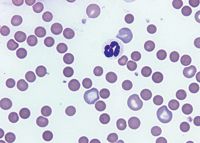
1. A peripheral blood smear from an anemic dog reveals that the majority of the RBCs are small, dark, and lack central pallor, which indicates they are spherocytes. Several large polychromatophilic cells are also present, which indicate a regenerative response to the anemia (Wright's-Giemsa stain; 1000X)
1. 貧血犬隻的外周血液抹片顯示,大多數紅血球呈現體積小、顏色深且缺乏中央蒼白區,此為球形紅血球特徵。同時可見數個大型多染性細胞,表明對貧血產生的再生性反應(Wright-Giemsa 染色;1000 倍)
Direct Coombs test 直接庫姆斯試驗
The direct Coombs test, also called the direct antiglobulin test, can be used when IMHA is suspected but autoagglutination is not seen. This test is run on an EDTA blood sample and will identify antibodies or complement on a patient's RBC surface.
直接庫姆斯試驗又稱直接抗球蛋白試驗,當懷疑 IMHA 但未觀察到自體凝集現象時可使用此檢測。該檢測採用 EDTA 抗凝血樣本進行,可識別患者紅血球表面存在的抗體或補體。
A positive result on a direct Coombs test does not distinguish between primary and secondary causes of IMHA.1 False positive results are seen in both dogs and cats and can be a result of concurrent diseases such as neoplasia, infections, inflammatory conditions, or recent drug administration.15 False negative results are also common and can occur in up to 42% of all dogs with IMHA.16 Thus, this test can be prone to errors and is not sensitive enough to detect low levels of clinically relevant antibodies.9 Flow cytometry also detects antierythrocyte antibodies and is more sensitive for detecting IgG than is the Coombs test, but it is not yet widely available to general practitioners.15,17
直接庫姆斯試驗(Direct Coombs test)呈陽性結果並不能區分 IMHA 是原發性或繼發性病因。1 在犬貓中均可能出現假陽性結果,這可能與併發疾病有關,例如腫瘤、感染、炎症狀況或近期用藥史。15 假陰性結果也很常見,在所有罹患 IMHA 的犬隻中發生率可達 42%。16 因此,該檢測容易出現誤差,且對於檢測臨床相關的低濃度抗體敏感度不足。9 流式細胞術也能檢測抗紅血球抗體,且對 IgG 的檢測靈敏度高於庫姆斯試驗,但目前尚未普及至一般臨床獸醫師使用。15,17


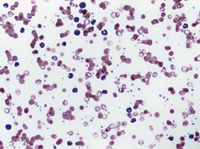
2. A peripheral blood smear from an anemic dog reveals that the RBCs are prominently clumped together, which indicates agglutination. A saline dispersion test should be performed for confirmation.
2. 貧血犬隻的外周血液抹片顯示紅血球明顯聚集,表明存在凝集現象。應進行生理鹽水分散試驗以確認診斷。
Additional findings in this smear include moderate polychromasia and rare nucleated RBCs, which indicate a regenerative response, small round cells lacking central pallor suggestive of spherocytes, and a neutrophilic leukocytosis, which indicates inflammation (Wright's-Giemsa stain; 500X).
該抹片的其他發現包括中度多染性紅血球症和少量有核紅血球,顯示再生性反應;缺乏中央蒼白區的小圓形細胞(符合球形紅血球特徵);以及中性粒細胞增多症,表明存在炎症反應(Wright-Giemsa 染色;500 倍放大)。
Imaging 影像學檢查
Obtain abdominal radiographs to investigate triggers of hemolytic anemia, such as ingestion of zinc-containing foreign objects or abdominal neoplasia. If abdominal radiographs reveal suspicious findings, an abdominal ultrasonographic examination is warranted.
進行腹部 X 光攝影以調查溶血性貧血的誘發因素,例如攝入含鋅異物或腹部腫瘤。若腹部 X 光顯示可疑發現,則需進行腹部超音波檢查。
In middle-aged to older dogs, it is recommended that routine thoracic radiographs also be obtained to investigate whether primary or metastatic neoplasia may be a cause of IMHA.
對於中老年犬隻,建議同時進行常規胸腔 X 光攝影,以調查原發性或轉移性腫瘤是否可能為免疫媒介性溶血性貧血(IMHA)的病因。
Other diagnostic tests 其他診斷檢測
A thorough search for underlying infection is warranted in cases of IMHA. Chronic infections, such as pyometra, abscesses, urinary tract infections, and discospondylitis, have all been associated with triggering IMHA.1 Transmissible causes of IMHA, such as infection with the hemoprotozoan Babesia gibsoni, are increasingly frequent in the United States.18 A recent study described a breed predisposition to B. gibsoni infection in American pit bull terriers.18 Studies have also described transmission associated with blood transfusions and dog bites.19-21 Other infectious organisms, such as Ehrlichia and Dirofilaria species, have also been associated with anemia in dogs.22,23 Mycoplasmosis does not cause a clinically relevant anemia in dogs that have not undergone a splenectomy, but it can cause a mild to severe anemia in cats.1
對於免疫媒介溶血性貧血(IMHA)病例,必須徹底排查潛在感染。慢性感染如子宮蓄膿、膿腫、泌尿道感染和椎間盤炎都與引發 IMHA 有關。1 在美國,可傳播的 IMHA 病因(例如感染血原蟲巴貝斯蟲 Babesia gibsoni)正日益頻繁。18 最近一項研究指出美國比特鬥牛梗對 B. gibsoni 感染具有品種易感性。18 研究也記載了與輸血和犬咬傷相關的傳播途徑。19-21 其他感染性病原體如艾利希體屬和犬心絲蟲也與犬隻貧血有關。22,23 支原體病在未接受脾切除術的犬隻中不會引起臨床相關貧血,但可能導致貓隻出現輕度至重度貧血。1
A coagulation panel is justified to investigate blood loss as a cause of anemia or as an indicator of disseminated intravascular coagulation (DIC).24 Elevations in coagulation times, however, have not been shown to predict thromboembolism or mortality in patients with IMHA.
凝血功能檢查對於調查貧血是否由失血引起,或作為彌散性血管內凝血(DIC)的指標是必要的。24 然而,凝血時間延長尚未被證實能預測 IMHA 患者的血栓栓塞或死亡率。
In one study in dogs with IMHA, no statistical difference was noted in survival times in patients with or without baseline coagulation abnormalities.25
在一項針對患有 IMHA 的犬隻研究中,有或無基礎凝血功能異常的患者其存活時間並無統計學上的顯著差異。25
An antinuclear antibody (ANA) test is occasionally performed in patients with IMHA to investigate systemic lupus erythematosus; but to truly have this condition, patients must have high ANA titers and two or more manifestations of autoimmunity (e.g. dermatomyositis, vasculitis, polyarthropathy) in addition to IMHA.26 False positive results can occur with certain underlying infections and neoplastic diseases.
抗核抗體(ANA)檢測偶爾會對 IMHA 患者進行,以調查全身性紅斑狼瘡;但要確診此病症,患者除了 IMHA 外,還必須具有高 ANA 效價及兩種以上自體免疫表現(例如皮肌炎、血管炎、多關節病)。26 某些潛在感染和腫瘤性疾病可能導致假陽性結果。
A bone marrow aspirate or core biopsy may be helpful in an ongoing nonregenerative anemia to search for underlying diseases such as RBC aplasia or hypoplasia, immune destruction of RBC precursors, or neoplastic infiltration.24
對於持續性非再生性貧血,骨髓穿刺或核心活檢可能有助於尋找潛在疾病,例如紅血球再生不良或發育不全、紅血球前驅細胞的免疫性破壞,或腫瘤浸潤。24
TREATMENT IN DOGS 犬隻治療方案
The decision to hospitalize a patient with IMHA depends largely on the severity of clinical signs. If the disease is caught early and the patient is stable, close outpatient management can be a reasonable option. More often, patients presenting with IMHA are already quite sick and need hospitalization for monitoring, supportive care, and treatment.
是否讓 IMHA 病患住院主要取決於臨床症狀的嚴重程度。若疾病早期發現且病患狀況穩定,密切的門診管理可能是合理的選擇。但多數情況下,出現 IMHA 症狀的病患通常已經相當虛弱,需要住院進行監測、支持性照護和治療。
The treatment of IMHA is extremely case-specific but generally involves four principles: 1) preventing hemolysis with immunosuppressive therapy, 2) treating tissue hypoxia, 3) deterring the formation of thromboemboli, and 4) providing supportive care.
IMHA 的治療極度個案化,但通常遵循四大原則:1)使用免疫抑制療法防止溶血 2)治療組織缺氧 3)預防血栓形成 4)提供支持性照護。
Immunosuppressive therapy
免疫抑制療法
Numerous drugs have been described to treat IMHA (Table 3). The first line of treatment in IMHA is immunosuppressive corticosteroids.
有多種藥物可用於治療 IMHA(表 3)。IMHA 的第一線治療是免疫抑制性皮質類固醇。
The addition of secondary and tertiary immunosuppressants may be indicated when patients present with severe IMHA (very low hematocrits, severe autoagglutination, intravascular hemolysis, or thrombocytopenia), when glucocorticoids do not adequately control the hemolysis, or when the side effects of glucocorticoids become unacceptable.
當病患出現嚴重的免疫媒介性溶血性貧血(IMHA)(如極低血球容積比、嚴重自體凝集、血管內溶血或血小板減少症)、糖皮質激素無法有效控制溶血,或糖皮質激素的副作用變得難以接受時,可能需要添加二線和三線免疫抑制劑。
The use of multiple cytotoxic drugs in combination requires careful monitoring, however, as there is a risk of severe immunosuppression and danger of infection.27
然而,合併使用多種細胞毒性藥物需要謹慎監測,因為存在嚴重免疫抑制和感染風險的危險。27



Table 3: Immunosuppressive Drugs Used to Treat IMHA in Dogs
表 3:用於治療犬隻 IMHA 的免疫抑制藥物
Corticosteroids. Dexamethasone (0.1 to 0.3 mg/kg intravenously once or twice daily) can be given initially if oral medications cannot be tolerated. Prednisone or prednisolone (2 mg/kg orally once or twice daily) is the oral drug of choice.
皮質類固醇。若無法耐受口服藥物,初期可靜脈注射地塞米松(每日 1-2 次,每次 0.1 至 0.3 mg/kg)。潑尼松或潑尼松龍(每日 1-2 次,每次 2 mg/kg 口服)是首選的口服藥物。
Glucocorticoids are thought to prevent hemolysis by decreasing the clearance of antibody-coated RBCs by macrophages, reducing the amount of antibody binding and complement activation on RBCs, and, in the long-term, minimizing autoantibody production.1 Side effects include polyuria, polydipsia, polyphagia, increased panting, gastrointestinal ulceration, and increased susceptibility to infection.
糖皮質激素被認為可通過以下機制防止溶血:減少巨噬細胞對抗體包被紅細胞的清除、降低紅細胞上抗體結合與補體激活的程度,以及長期使用可最小化自身抗體的生成。1 副作用包括多尿、煩渴、多食、呼吸急促增加、胃腸道潰瘍形成及感染易感性增加。
Azathioprine. In cases of severe IMHA (low RBC counts, autoagglutination, or intravascular hemolysis), the second drug usually added in dogs is azathioprine (2 mg/kg orally once daily or every other day).
硫唑嘌呤。對於嚴重免疫介導性溶血性貧血(紅細胞計數低、自體凝集或血管內溶血)的病例,犬隻通常會加用的第二種藥物是硫唑嘌呤(口服 2 毫克/公斤,每日一次或隔日一次)。
Studies have shown increased survival times in dogs treated with glucocorticoids and azathioprine.13,28 Drawbacks to this medication are that it is only available in oral form and it can take weeks to take effect.
研究顯示,接受糖皮質激素與硫唑嘌呤聯合治療的犬隻存活時間顯著延長。13,28 此藥物的缺點在於僅有口服劑型,且需數週才能顯現療效。
Azathioprine is a purine analogue antimetabolite that disrupts DNA and RNA synthesis and is effective in limiting cell-mediated immunity (T-lymphocyte function).24 Side effects can include gastrointestinal upset, bone marrow suppression, pancreatitis, and hepatotoxicity.
硫唑嘌呤是一種嘌呤類似物抗代謝藥,可干擾 DNA 與 RNA 合成,並能有效抑制細胞介導免疫(T 淋巴細胞功能)。24 可能產生的副作用包括胃腸道不適、骨髓抑制、胰腺炎及肝毒性。
Regular physical examinations and complete blood counts and serum chemistry profiles (weekly at first, then monthly) will help to monitor for the more serious complications of this medication. Azathioprine can cause severe bone marrow and hepatic toxicosis in cats and is not recommended.24
定期進行身體檢查、全血球計數及血清生化檢查(初期每週一次,之後每月一次)有助於監測此藥物可能引起的嚴重併發症。Azathioprine 可能導致貓咪出現嚴重的骨髓與肝臟毒性,因此不建議使用於貓科動物。24
Cyclosporine. A third drug gaining acceptance in treating IMHA is cyclosporine (2.5 to 5 mg/kg orally twice daily). An intravenous form is available, but no clinical trials with this form have been published in the veterinary literature.
環孢素。第三種獲得認可用於治療 IMHA 的藥物是環孢素(口服劑量為每日兩次,每次 2.5 至 5 毫克/公斤)。雖有靜脈注射劑型,但獸醫文獻中尚未發表相關臨床試驗報告。
The one retrospective study that investigated cyclosporine (which was given at a slightly higher than recommended dosage) showed no benefit compared with other drug protocols.29
一項針對環孢素(使用劑量略高於建議劑量)的回顧性研究顯示,與其他藥物治療方案相比並無顯著優勢。29
Cyclosporine is a potent T-cell suppressor that blocks production of immune activating factors in both T-helper cells and T-cytotoxic cells, as well as blocks the expression of IL-2 and gamma-interferon. The outcome is a reduction of cell-mediated immunity and antibody production.
環孢素是一種強效 T 細胞抑制劑,能同時阻斷輔助性 T 細胞與細胞毒性 T 細胞中免疫激活因子的產生,並抑制 IL-2 與γ-干擾素的表現。其作用結果是降低細胞介導免疫反應與抗體生成。
Side effects include gastrointestinal upset, gingival hyperplasia (can regress with dose tapering), increased susceptibility to infection, and lethargy.
副作用包括胃腸不適、牙齦增生(劑量遞減後可能改善)、感染風險增加以及嗜睡。
Although it is recommended that cyclosporine concentrations are measured every two to four weeks (maintaining trough concentrations, depending on the method used, between 100 and 300 ng/ml), it is now questionable whether blood concentrations of this drug need to be measured if clinical disease is well-controlled.17
雖然建議每兩到四周測量一次環孢素濃度(根據檢測方法不同,維持谷濃度在 100 至 300 ng/ml 之間),但若臨床症狀控制良好,目前對於是否需要監測此藥物血中濃度仍存在疑問。17
Cyclophosphamide. In addition to the above therapeutic options, a handful of other medications have been used with varying degrees of success. Cyclophosphamide, an alkylating agent that suppresses the immune system, can be given as a single intravenous or oral dose initially in the course of treatment (200 mg/m2 ) or as a four days on/three days off (50 mg/m2 /day) protocol.
環磷醯胺。除上述治療選擇外,尚有少數其他藥物曾被使用並取得不同程度的成效。環磷醯胺作為一種烷化劑,可抑制免疫系統,可在治療初期以單次靜脈或口服劑量(200 mg/m2)給藥,或採用四天給藥/三天停藥(每日 50 mg/m2)的治療方案。
Cyclophosphamide harms B and T cells by cross-linking DNA, inhibiting humoral and cell-mediated immunity, and suppressing neutrophil and macrophage function. Side effects include gastrointestinal upset, myelosuppression, and hemorrhagic cystitis. Because of the severity of some of these signs, cyclophosphamide is not widely used in the long-term treatment of IMHA.
環磷醯胺會透過交聯 DNA 來傷害 B 細胞和 T 細胞,抑制體液免疫和細胞介導免疫,並抑制中性球和巨噬細胞功能。副作用包括胃腸不適、骨髓抑制和出血性膀胱炎。由於部分症狀可能相當嚴重,環磷醯胺並未被廣泛用於 IMHA 的長期治療。
Instead, it is commonly used in early treatment of severe refractory IMHA.
相反地,它通常用於治療嚴重難治性 IMHA 的早期階段。
Cyclophosphamide has fallen out of favor since a randomized, controlled, prospective clinical trial published in 2003 showed no improved recovery or survival times in patients treated with cyclophosphamide and prednisone vs. prednisone alone.30 Many other studies have also documented decreased survival in patients treated with cyclophosphamide.13,29,30
自 2003 年一項隨機對照前瞻性臨床試驗發表後,環磷醯胺已逐漸失寵,該研究顯示使用環磷醯胺合併 prednisone 治療的患者,其康復率或存活時間並未優於單獨使用 prednisone 的患者 30。許多其他研究也記錄了使用環磷醯胺治療患者存活率下降的情況 13,29,30。
Mycophenolate mofetil. Mycophenolate mofetil (10 to 20 mg/kg orally or intravenously twice daily), similar to azathioprine, targets B and T lymphocytes by inhibiting an enzyme necessary for de novo purine biosynthesis.15 This drug was developed to help prevent allograft rejection in people and has been used in dogs to treat myasthenia gravis and glomerulonephritis.
黴酚酸酯。黴酚酸酯(口服或靜脈注射,每日兩次,每次 10 至 20 毫克/公斤)與 azathioprine 類似,透過抑制嘌呤從頭合成所需的酵素來針對 B 細胞和 T 淋巴細胞 15。這種藥物最初是為了幫助預防人類同種異體移植排斥而開發,並已被用於治療犬的重症肌無力和腎小球腎炎。
At therapeutic doses, mycophenolate is minimally myelosuppressive, but gastrointestinal side effects can be substantial in dogs (gastrointestinal hemorrhage, anorexia, and diarrhea).
在治療劑量下,黴酚酸酯的骨髓抑制作用極小,但可能對犬隻造成顯著的胃腸道副作用(胃腸道出血、厭食和腹瀉)。
To minimize these side effects, the dose can be lowered to well-tolerated levels when used in conjunction with other myelosuppressive drugs.31 Few reports have been published on the use of this drug for IMHA.32
為減輕這些副作用,當與其他骨髓抑制藥物併用時,可將劑量降低至耐受良好的水平。31 目前關於此藥物用於治療 IMHA 的報告相當有限。32
Danazol. Danazol (5 mg/kg orally two to three times daily), a synthetic androgen, has been used to treat
達那唑。達那唑(口服 5 毫克/公斤,每日兩至三次)是一種合成雄性激素,已被用於治療
immune-mediated disease in people and is sometimes recommended in addition to standard therapies to treat IMHA in dogs.
人類的自體免疫疾病,有時會建議作為標準療法的輔助治療用於犬隻的 IMHA。
Danazol likely exerts its immunomodulatory effects by decreasing the production of IgG and cytokines, inhibiting complement activation, and reducing the binding of antibody and complement to erythrocytes.24 Danazol is not widely used for three main reasons: it is expensive, it can take weeks to observe a clinical response, and it is potentially hepatotoxic.1 While one study did not show improved outcome with this drug, the small number of reports in the veterinary literature makes the use of this drug difficult to assess.33
丹那唑可能通過以下機制發揮其免疫調節作用:減少 IgG 和細胞因子的產生、抑制補體活化,以及降低抗體和補體與紅血球的結合。24 丹那唑未被廣泛使用主要有三個原因:價格昂貴、需數週才能觀察到臨床反應,以及具有潛在肝毒性。1 雖然一項研究未顯示該藥物能改善治療結果,但獸醫文獻中相關報告數量稀少,使得此藥物的療效難以評估。33
Leflunomide. Leflunomide (4 mg/kg orally once daily), an inhibitor of pyrimidine biosynthesis, has been used to treat rheumatoid arthritis in people and granulomatous meningoencephalomyelitis, neoplasia, and graft rejection in dogs. Limited but favorable reports exist on the use of this drug for treating IMHA.
來氟米特。來氟米特(口服每日一次,4 毫克/公斤)是一種嘧啶生物合成抑制劑,已用於治療人類類風濕性關節炎,以及犬的肉芽腫性腦膜腦炎、腫瘤和移植排斥反應。目前有限但正向的報告顯示此藥物可用於治療免疫介導性溶血性貧血。
Side effects in dogs appear to be minimal but can include vomiting, lymphopenia, and anemia. The recent introduction of a generic form may make it less costly for routine treatment. The dose should be adjusted to maintain a serum trough concentration of 20 µg/ml.31
犬隻使用後的副作用似乎較輕微,但可能包括嘔吐、淋巴球減少和貧血。近期推出的學名藥可能降低常規治療成本。應調整劑量以維持血清谷濃度 20 微克/毫升。31
IVIG. Intravenous human immunoglobulin (IVIG) (0.5 to 2 g/kg intravenously daily, given over six to 12 hours) has been infrequently used to treat a variety of immune-mediated diseases in dogs, including IMHA.
靜脈注射人類免疫球蛋白(IVIG)(每日靜脈注射 0.5 至 2 g/kg,持續 6 至 12 小時)在犬隻中偶爾被用於治療多種免疫介導疾病,包括免疫介導溶血性貧血(IMHA)。
The mechanism of action of IVIG is thought to be a blockade of the Fc receptors on macrophages, thereby reducing phagocytosis of antibody-coated RBCs, interfering with complement, and suppressing antibody production.
IVIG 的作用機制被認為是阻斷巨噬細胞上的 Fc 受體,從而減少抗體包被紅血球的吞噬作用、干擾補體系統並抑制抗體產生。
In addition, IVIG inhibits erythrocyte phagocytosis by binding to canine monocytes and lymphocytes and possibly by an anti-idiotypic down-regulation of antibody production.
此外,IVIG 通過與犬單核細胞和淋巴細胞結合,並可能通過抗獨特型抗體產生的下調作用,來抑制紅血球吞噬作用。
IVIG can be given to patients with IMHA as a single infusion or on two or three consecutive days.34 Although IVIG appears to impart short-term benefits (reflected by a rising packed cell volume and reticulocytosis) within days of infusion, long-term benefits were not seen. No complications have been seen with a single IVIG infusion in dogs.
IVIG 可對 IMHA 患者進行單次輸注或在連續兩至三天內使用。雖然 IVIG 在輸注後數天內似乎能帶來短期效益(表現為血球容積比上升和網織紅血球增多),但未觀察到長期效益。在犬隻中單次 IVIG 輸注未見併發症。
Unfortunately, IVIG is also costly and difficult to obtain.30
不幸的是,靜脈注射免疫球蛋白(IVIG)不僅成本高昂且難以取得。30
Liposomal-encapsulated clodronate. Liposomal-encapsulated clodronate (dichloromethylene diphosphonate) is the focus of two studies, one of which is ongoing at Colorado State University.35,36 Clodronate is a bisphosphonate that, when incorporated into liposomes, is rapidly phagocytized by macrophages leading to apoptosis.
脂質體包覆氯膦酸鹽。脂質體包覆氯膦酸鹽(二氯亞甲基二磷酸鹽)是兩項研究的焦點,其中一項正在科羅拉多州立大學進行中。35,36 氯膦酸鹽是一種雙磷酸鹽類藥物,當被包裹進脂質體後,會迅速被巨噬細胞吞噬並導致其凋亡。
Intravenous liposomal-encapsulated clodronate has been shown to significantly reduce the number of canine splenic macrophages and dendritic cells in vitro, thereby obstructing the clearance of antibody-coated RBCs. This reduction, in effect, slows the clearance of opsonized erythrocytes and allows time for the other immunosuppressive drugs to work.
研究顯示,靜脈注射脂質體包覆氯膦酸鹽能顯著減少犬隻脾臟巨噬細胞和樹突細胞的數量(體外實驗),從而阻斷抗體包覆紅血球的清除過程。這種減少作用實際上減緩了調理化紅血球的清除速度,為其他免疫抑制藥物發揮作用爭取了時間。
The initial study, involving intravenous infusion of liposomal-encapsulated clodronate in healthy dogs and in seven dogs with IMHA, found that the drug is rapid-acting and well-tolerated.35 In that study, results were favorable, and dogs treated with liposomal-encapsulated clodronate in conjunction with prednisone, azathioprine, and heparin demonstrated an improved survival.
最初的研究針對健康犬隻和七隻罹患 IMHA 的犬隻進行靜脈輸注脂質體包覆氯膦酸鹽,結果顯示該藥物起效快速且耐受性良好。35 該研究中,治療結果令人滿意,接受脂質體包覆氯膦酸鹽聯合潑尼松、硫唑嘌呤和肝素治療的犬隻表現出更高的存活率。
Splenectomy 脾臟切除術
Splenectomy is considered one of the last-choice treatments in canine IMHA.
脾臟切除術被視為犬隻免疫介導性溶血性貧血(IMHA)的最後治療選擇之一。
The benefits arise from removing one source of B cells and splenic macrophages, the primary culprits in the removal of antibody-coated erythrocytes.24 It is undetermined how effective this procedure is in routine IMHA cases, since only one recent clinical study has been done to assess it as a forerunner of treatment.37 Although this study did show increased survival with splenectomy (58% survival vs.
此手術的益處在於移除 B 細胞和脾臟巨噬細胞的來源,這些細胞是清除抗體包覆紅血球的主要元兇。24 目前尚不確定此手術在常規 IMHA 病例中的效果,因為僅有一項近期臨床研究將其作為治療先驅進行評估。37 雖然該研究確實顯示脾臟切除術可提高存活率(58%存活率 vs.
37.5% in the control group), the sample size was small.
對照組 37.5%),但樣本數較小。
Consider splenectomy only in patients that have not responded to immunosuppressive medications, require high-dose and long-term medications to maintain a remission, or are experiencing severe side effects from medications. As there is a risk of developing marked infection after splenectomy, it is not recommended for patients taking multiple immunosuppressive medications.1
僅對以下患者考慮脾切除術:對免疫抑制藥物無反應、需要高劑量長期用藥才能維持緩解,或正經歷藥物嚴重副作用者。由於脾切除後有發生顯著感染的風險,不建議正在服用多種免疫抑制藥物的患者接受此手術。1
Treating tissue hypoxia 治療組織缺氧
Patients with IMHA often need oxygen-carrying fluids to support them through the first few days of care until immunosuppression begins to control the disease process. Oxygen alone is rarely beneficial in severe anemia, unless a patient's clinical signs are complicated by thromboembolism.
IMHA 患者通常需要輸注攜氧液體以支持最初幾天的治療,直到免疫抑制開始控制疾病進程。單獨給氧在嚴重貧血中很少有益,除非患者的臨床症狀因血栓栓塞而複雜化。
The criteria for transfusion are not rigid but may include the presence of severe tachypnea, dyspnea, tachycardia, cold extremities, weakness, mental depression, or a hematocrit under 15%.
輸血標準並非嚴格固定,但可能包括以下情況:出現嚴重呼吸急促、呼吸困難、心動過速、四肢冰冷、虛弱、精神抑鬱,或血球容積比低於 15%。
If a patient appears comfortable when resting in a cage but becomes agitated and clinically unstable during necessary procedures (radiography or ultrasonography), give a transfusion before proceeding.
若病患在籠內休息時表現舒適,但在必要檢查程序(放射攝影或超音波檢查)期間出現躁動且臨床狀態不穩定,應在進行檢查前先給予輸血治療。
The choice of administering packed RBCs, whole blood, or synthetic hemoglobin can be controversial and is often institution-dependent. Ideally, only the necessary component should be given. As transfusion reactions can occur in patients that have not had transfusions previously, crossmatching should be done before transfusion in all non-autoagglutinating patients.
選擇輸注濃縮紅血球、全血或合成血紅素可能具有爭議性,通常取決於醫療機構的常規。理想情況下應僅輸注必要成分。由於未曾接受輸血的病患仍可能發生輸血反應,所有未出現自體凝集現象的病患在輸血前都應進行交叉配對試驗。
Also perform cross-matching in any dog that has received a prior blood transfusion.
對於曾接受過輸血的犬隻,也應執行交叉配對試驗。
Since autoagglutination may interfere with accurate blood typing and crossmatching, packed RBCs should only be administered from universal donors (DEA 1-7 negative blood; DEA 4 can be positive) in dogs with IMHA.15 Administering purified polymerized bovine hemoglobin solution (Oxyglobin—Biopure) can be beneficial in cases in which crossmatching is not possible or compatible blood is not available.
由於自體凝集可能影響血型鑑定與交叉配對的準確性,對於罹患免疫媒介性溶血性貧血(IMHA)的犬隻,應僅使用通用供血者(DEA 1-7 陰性血液;DEA 4 可為陽性)的濃縮紅血球進行輸注。當無法進行交叉配對或缺乏相容血液時,輸注純化聚合牛血紅素溶液(Oxyglobin—Biopure)可能有所助益。
Although one study noted that Oxyglobin administration was associated with a poorer prognosis, a more recent study contradicted those findings.12,29
雖然一項研究指出 Oxyglobin 的施用與較差的預後相關,但一項更近期的研究反駁了這些發現。12,29
Thromboembolism and anticoagulants
血栓栓塞與抗凝血劑
DIC and thromboembolism are common causes of morbidity and mortality in patients with IMHA.1 The pathogenesis is largely unknown, but potential contributors include endogenous conditions such as blood flow stasis and hypercoaguability as well as exogenous factors such as repeated venipuncture, intravenous catheters, and glucocorticoid administration.
瀰漫性血管內凝血(DIC)和血栓栓塞是 IMHA 患者發病率和死亡率的常見原因。1 其發病機制尚不清楚,但可能的誘因包括內源性因素如血流淤滯和高凝狀態,以及外源性因素如反覆靜脈穿刺、靜脈導管和糖皮質激素的施用。
Whether anticoagulant therapy is used at the time of diagnosis or added when thromboembolism is suspected is largely institution-dependent.
是否在診斷時就使用抗凝血治療,或是在懷疑血栓栓塞時才追加使用,主要取決於各醫療機構的常規做法。
Anticoagulants such as low-molecular-weight heparin, unfractionated heparin, warfarin, low-dose aspirin, and fresh-frozen plasma have all been used to prevent or treat this condition, although few studies have shown prolonged survival with their use.15
諸如低分子量肝素、未分餾肝素、華法林、低劑量阿司匹林以及新鮮冷凍血漿等抗凝血劑,均曾被用於預防或治療此病症,然而鮮少研究顯示這些藥物能延長存活期。15
In one study, the use of fresh-frozen plasma (10 ml/kg) with unfractionated heparin (100 U/kg subcutaneously every six hours) failed to prevent thromboembolic complications in IMHA patients.38 Unfractionated heparin alone is generally not associated with an increased risk of bleeding, but neither is it associated with an improved outcome.
一項研究顯示,使用新鮮冷凍血漿(10 毫升/公斤)配合未分餾肝素(每六小時皮下注射 100 單位/公斤)並未能預防 IMHA 患者的血栓栓塞併發症。38 單獨使用未分餾肝素通常不會增加出血風險,但也無助於改善預後。
Two studies failed to document increased survival with the use of unfractionated heparin.13,14 Another study demonstrated that relatively high doses of unfractionated heparin (300 to 375 U/kg subcutaneously every six hours) were needed to obtain target concentrations for anticoagulation, and even those concentrations may be inadequate in preventing thrombosis.39 If used, unfractionated heparin should be adjusted to prolong the activated partial thromboplastin time to 25% to 50% over baseline or to inhibit factor Xa to a target range of 0.35 to 0.7 U/ml.
兩項研究未能證實使用未分餾肝素可提高存活率。13,14 另一項研究則表明,需要相對高劑量的未分餾肝素(每六小時皮下注射 300 至 375 單位/公斤)才能達到抗凝血目標濃度,且即使達到該濃度仍可能不足以預防血栓形成。39 若使用未分餾肝素,應調整劑量使活化部分凝血活酶時間延長至基準值的 25%至 50%,或將 Xa 因子抑制至 0.35 至 0.7 單位/毫升的目標範圍。
Low-molecular-weight heparin (150 to 200 U/kg subcutaneously every six to eight hours) is an alternative to unfractionated heparin and is starting to be used to treat thromboembolic disease in veterinary medicine.
低分子量肝素(每 6 至 8 小時皮下注射 150 至 200 U/kg)是未分餾肝素的替代藥物,已開始用於獸醫領域治療血栓栓塞性疾病。
Low-molecular-weight heparins have better subcutaneous bioavailability, are better able to inhibit factor Xa, and likely can be given at a decreased frequency compared with unfractionated heparin. No clinical studies have been done to determine whether this drug is effective in preventing thromboembolism in patients with IMHA.
與未分餾肝素相比,低分子量肝素具有更好的皮下生物利用度,能更有效抑制 Xa 因子,且可能減少給藥頻率。目前尚無臨床研究證實此藥物對預防 IMHA 患者血栓栓塞是否有效。
Measuring anti-Xa activity is necessary to monitor the anticoagulant effects of this drug.
必須測量抗 Xa 活性來監測此藥物的抗凝血效果。
The use of ultra low-dose aspirin (0.5 mg/kg orally once daily) in addition to immunosuppressive medications has shown clear promise in canine patients. The beneficial effects of aspirin are thought to be from vasodilation and modulation of platelet aggregation.
在免疫抑制藥物之外併用超低劑量阿斯匹靈(每日口服 0.5 mg/kg)已顯示對犬病患具有明確療效。阿斯匹靈的益處被認為來自血管擴張作用及調節血小板聚集。
One large study in dogs treated with glucocorticoids and azathioprine compared the use of ultra low-dose aspirin, unfractionated heparin, and a combination of these two medications.14 The results demonstrated that the patients treated with aspirin had significantly longer survival times than patients treated with unfractionated heparin alone.
一項針對接受糖皮質激素和硫唑嘌呤治療犬隻的大型研究,比較了超低劑量阿司匹林、未分餾肝素以及這兩種藥物組合使用的效果。14 研究結果顯示,接受阿司匹林治療的患者其存活時間明顯長於僅接受未分餾肝素治療的患者。
In this study, the use of aspirin was not associated with any adverse clinical effects, even when used with high-dose glucocorticoids.
在這項研究中,阿司匹林的使用並未導致任何不良臨床反應,即使與高劑量糖皮質激素併用時也是如此。
Supportive care 支持性照護
Aggressive, detail-oriented supportive care is a critical factor for the successful treatment of IMHA. Timely recognition and treatment of an underlying disease can allow immunosuppressive drug therapy to be tapered more quickly. Antibiotic administration while awaiting confirmation of suspected infectious disease can improve the chances of recovery.
積極且注重細節的支持性照護是成功治療免疫介導性溶血性貧血(IMHA)的關鍵因素。及時發現並治療潛在疾病可讓免疫抑制藥物治療更快減量。在等待疑似感染性疾病確診期間給予抗生素治療,可提高康復機率。
Thorough diagnostic testing can help detect underlying infectious or neoplastic causes of immune-mediated hemolysis, which if missed would make treatment unlikely to succeed. Finally, the quick detection of complications and the speedy removal of nonessential drugs that can cause an immune reaction can also help improve the chances of survival.
徹底的診斷檢測有助於發現潛在的感染性或腫瘤性病因所導致的免疫介導性溶血,若未能發現這些病因將使治療難以成功。最後,快速發現併發症並及時停用可能引發免疫反應的非必要藥物,也能提高存活機會。
Good nursing care that includes daily intravenous catheter care, proper nutrition, short walks, low-stress handling, and limited phlebotomy can also contribute to a better outcome. Peripheral intravenous catheter placement may be preferable to jugular placement in patients with the potential to develop a coagulopathy.
良好的護理照護包括每日靜脈導管護理、適當營養、短程散步、低壓力操作及限制抽血次數,這些都有助於改善預後。對於可能出現凝血功能障礙的病患,選擇周邊靜脈導管置放可能比頸靜脈置放更為合適。
Ancillary treatments and medications such as intravenous fluids, gastric protectants, promotility drugs, and antinausea medications can all support a patient through the initial days of treatment. Intravenous fluids, especially in patients with intravascular hemolysis, may help prevent hemogloblin nephrosis.
輔助治療與藥物如靜脈輸液、胃黏膜保護劑、促腸胃蠕動藥物及止吐藥物,都能支持病患度過治療初期。靜脈輸液對於血管內溶血病患尤其重要,可能有助於預防血紅素腎病變。
Removing unnecessary indwelling catheters may reduce the risks of thromboembolism.15
移除非必要的留置導管可降低血栓栓塞風險。15
LONG-TERM MANAGEMENT AND PROGNOSIS
長期管理與預後
A steady or rising hematocrit, increasing reticulocytes, and decreasing spherocytes indicate a positive response to therapy.1 Medication tapering usually does not begin until the hematocrit is normal. Tailor drug tapering to the individual patient. Glucocorticoids can be tapered by about 25% every three to four weeks.
穩定的或上升的血球容積比、增加的網狀紅血球以及減少的球形紅血球,顯示對治療有正面反應。1 藥物減量通常要等到血球容積比恢復正常才開始。藥物減量應根據個別病患情況調整。糖皮質激素可每三至四周減少約 25%的劑量。
If an underlying disease has been addressed or the response to treatment is rapid, drug tapering can occur more quickly. Measure the hematocrit five to seven days after discharge and again after each decrease in drug dosage.
若潛在疾病已得到控制或對治療反應迅速,藥物減量可進行得更快。出院後五至七天應測量血球容積比,之後每次藥物劑量減少時也需再次測量。
Perform a complete blood count, reticulocyte count, blood smear, serum chemistry profile, urinalysis, and urine culture every four to eight weeks as needed to monitor for drug side effects, infections, and disease relapse.
視需要每四至八週進行全血球計數、網狀紅血球計數、血液抹片檢查、血清生化檢查、尿液分析及尿液培養,以監測藥物副作用、感染及疾病復發情況。
A recent study documented that about three months of therapy was sufficient in dogs successfully treated for IMHA, although a subset of dogs needed longer treatment.3 A written drug-tapering and recheck schedule can be provided for the owners to follow, under the supervision of a veterinarian.
最近一項研究記錄顯示,對於成功治療免疫介導性溶血性貧血(IMHA)的犬隻,約三個月的治療期即已足夠,不過有部分犬隻需要更長的治療時間。3 獸醫師可提供書面藥物漸減和複診時間表供飼主遵循。
After finishing all medications, rechecks should occur quarterly for a year, then biannually.
完成所有藥物治療後,第一年應每季進行複診,之後改為每半年一次。
Relapse of disease has been documented to be roughly 12% to 24%, although different protocols and studies make comparison difficult.3,13 If relapse occurs, reinstitute medications at high dosages and taper more slowly.
據文獻記載疾病復發率約為 12%至 24%,但由於不同治療方案和研究方法使得數據難以直接比較。3,13 若發生復發,應重新以高劑量給藥並採用更緩慢的漸減方案。
The mortality associated with IMHA is documented to be between 29% and 70%, with a large percentage of deaths occurring within the first two weeks of diagnosis.3 Predictors of increased mortality in dogs include increased blood urea nitrogen concentrations, decreased platelets, and petechiae at the time of diagnosis.
文獻記載 IMHA 相關死亡率介於 29%至 70%之間,其中大部分死亡病例發生在診斷後的頭兩週內。3 犬隻死亡率增加的預測因子包括:診斷時血尿素氮濃度升高、血小板減少以及出現瘀點。
Dogs that survive the first two weeks after diagnosis have a six-month survival rate of 92.5%.3
確診後存活超過兩週的犬隻,其六個月存活率可達 92.5%。3
CATS AND IMHA 貓與免疫介導性溶血性貧血
In cats, IMHA is most often secondary to feline leukemia virus (FeLV) or Mycoplasma haemofelis (formerly Haemobartonella felis) infection although it can also be seen with other infections (feline infectious peritonitis, Cytauxzoon felis infection), drug therapy (methimazole, propylthiouracil), toxins (onions), and neoplasia (lymphoma).40,41 One study documented no increased risk of IMHA in hospitalized cats given subcutaneous vs. intravenous famotidine.42
貓隻罹患免疫介導性溶血性貧血(IMHA)最常見的繼發性原因為貓白血病病毒(FeLV)或貓血黴漿菌(Mycoplasma haemofelis,舊稱 Haemobartonella felis)感染,但也可能與其他感染(貓傳染性腹膜炎、貓胞裂蟲症)、藥物治療(甲巰咪唑、丙硫氧嘧啶)、毒素(洋蔥)及腫瘤(淋巴瘤)有關。40,41 一項研究顯示,住院貓隻接受皮下或靜脈注射法莫替丁(famotidine)治療時,IMHA 發生風險並未增加。42
If you suspect IMHA in a cat based on history, clinical signs, and routine diagnostic test results, perform a FeLV test. Patients with FeLV infection often respond well initially to treatment but eventually succumb to the disease. Cats with M. haemofelis infection typically have recurrent episodes of hemolytic anemia. These organisms can sometimes be seen on a blood smear, although the best test is a PCR. Treat cats with antibiotics, immunosuppressive therapy, and blood transfusions as needed.1
若根據病史、臨床症狀及常規診斷結果懷疑貓隻患有 IMHA,應進行 FeLV 檢測。FeLV 感染病患初期治療反應通常良好,但最終仍會死於該疾病。感染貓血黴漿菌的貓隻通常會反覆發作溶血性貧血。這些病原體有時可透過血液抹片觀察,但最佳檢測方式為 PCR。治療方式包括抗生素、免疫抑制療法及必要時的輸血治療。1
Similar to dogs, cats with IMHA are initially started on immunosuppressive dosages of glucocorticoids. Little information is available describing the addition of secondary or tertiary immunosuppressive medications in cats with severe IMHA. Possible drugs to add include cyclosporine or cyclophosphamide.41
與犬隻類似,確診 IMHA 的貓咪最初會使用免疫抑制劑量的糖皮質激素進行治療。關於在嚴重 IMHA 貓咪中添加二線或三線免疫抑制藥物的相關資料相當有限。可考慮添加的藥物包括環孢素或環磷酰胺。41
CONCLUSION 結論
When IMHA is first identified, inform owners that the prognosis is variable, treatment is labor-intensive, hospitalization is expensive, and side effects from medications can be severe. Further, since RBC counts and overall stability are often erratic in these patients, prepare owners for the roller-coaster nature of this disease.
當首次診斷出 IMHA 時,應告知飼主預後情況多變、治療過程繁瑣、住院費用高昂,且藥物副作用可能相當嚴重。此外,由於這類病患的紅血球計數和整體狀況經常不穩定,需讓飼主做好心理準備,這將是一段如同雲霄飛車般的病程。
Owners also need to be prepared for frequent and costly recheck examinations.
飼主同時需準備面對頻繁且昂貴的複診檢查。
Although IMHA is a serious condition, patients can have a good prognosis if they respond to treatment, tolerate the side effects of medications needed for treatment, and do not succumb to secondary infections or thromboembolism.
雖然 IMHA 是一種嚴重的疾病,但如果患者對治療有反應、能夠耐受治療所需藥物的副作用,並且沒有因繼發性感染或血栓栓塞而死亡,預後可能良好。
The identification and treatment of underlying disease, the advent of new immunosuppressive drugs, and good supportive and owner care all contribute to increased survival in patients with IMHA.
基礎疾病的識別與治療、新型免疫抑制藥物的出現,以及良好的支持性照護與飼主護理,都有助於提高 IMHA 患者的存活率。
ACKNOWLEDGMENTS 致謝
Special thanks to Jennifer Neel, DVM, DACVP, assistant professor of clinical pathology, Department of Population Health and Pathobiology, College of Veterinary Medicine, North Carolina State University, for providing the photographs in this article.
特別感謝北卡羅來納州立大學獸醫學院人口健康與病理生物學系臨床病理學助理教授、獸醫學博士 Jennifer Neel(DVM, DACVP)提供本文照片。
Nicole Shaw, DVM, DACVIM Nicole Shaw, 獸醫學博士, 美國獸醫內科學院認證專科醫師
Veterinary Emergency and Referral Group
獸醫急診與轉診中心
318 Warren St. 華倫街 318 號
Brooklyn, NY 11201 紐約州布魯克林區, 郵遞區號 11201
Karyn Harrell, DVM, DACVIM
Karyn Harrell, 獸醫學博士, DACVIM
Department of Clinical Sciences
臨床科學系
College of Veterinary Medicine
獸醫學院
North Carolina State University
北卡羅來納州立大學
Raleigh, NC 27606 北卡羅來納州羅利市 27606
REFERENCES 參考文獻
1. Giger U. Regenerative anemias caused by blood loss or hemolysis. In: Ettinger SJ, Feldman EC. Textbook of veterinary internal medicine. 6th ed. St Louis, Mo: Elsevier Co, 2005;1886-1907.
1. Giger U. 由失血或溶血引起的再生性貧血。見:Ettinger SJ, Feldman EC. 《獸醫內科學教科書》第 6 版。密蘇里州聖路易斯:Elsevier Co, 2005;1886-1907.
2. Barker RN. Anemia associated with immune responses. In: Feldman BF, Zinkl JG, Jain NC, eds. Schalm's veterinary hematology. 5th ed. Philadelphia, Pa: Lippincott, Williams & Wilkins, 2000;169-175, 819-826.
2. Barker RN. 與免疫反應相關的貧血。見:Feldman BF, Zinkl JG, Jain NC 編.《Schalm 氏獸醫血液學》第 5 版。賓夕法尼亞州費城:Lippincott, Williams & Wilkins, 2000;169-175, 819-826.
3. Piek CJ, Junius G, Dekker A, et al. Idiopathic immune- mediated hemolytic anemia: treatment outcome and prognostic factors in 149 dogs. J Vet Intern Med 2008;22(2):366-373.
3. Piek CJ, Junius G, Dekker A 等. 特發性免疫介導溶血性貧血:149 隻犬的治療結果與預後因素。《獸醫內科醫學雜誌》2008;22(2):366-373.
4. Liang MM, Pfeiffer I, Roth T. The major histocompatibility complex and its role in canine immune-mediated hemolytic anemia and thrombocytopenia, in Proceedings. 16th European Coll Vet Intern Med Companion Anim Congress 2006.
4. Liang MM、Pfeiffer I、Roth T。《犬類主要組織相容性複合體及其在免疫介導性溶血性貧血與血小板減少症中的作用》,刊載於《第 16 屆歐洲獸醫內科醫學會伴侶動物大會論文集》2006 年。
5. Calvert CA, Sammarco C, Pickus C. Positive Coombs' test results in two dogs treated with amiodarone. J Am Vet Med Assoc 2000;216(12):1933-1936.
5. Calvert CA、Sammarco C、Pickus C。《兩隻接受胺碘酮治療犬隻出現庫姆斯試驗陽性結果》,刊於《美國獸醫學會雜誌》2000 年;216(12):1933-1936。
6. Van Israel N, French AT, Wotton PR, et al. Hemolysis associated with patent ductus arteriosis coil embolization in a dog. J Vet Intern Med 2001;15(2):153-156.
6. Van Israel N、French AT、Wotton PR 等。《犬隻動脈導管未閉線圈栓塞術相關溶血病例》,刊於《獸醫內科醫學期刊》2001 年;15(2):153-156。
7. Barker RN, Elson CJ. Red blood cell glycophorins as B and T-cell antigens in canine autoimmune haemolytic anemia. Vet Immunol Immunopathol 1995;47(3-4):225-238.
7. Barker RN、Elson CJ。《犬自體免疫溶血性貧血中紅血球糖蛋白作為 B 細胞與 T 細胞抗原之研究》,刊於《獸醫免疫學與免疫病理學》1995 年;47(3-4):225-238。
8. Barker RN, Gruffydd-Jones TJ, Stokes CR, et al. Autoimmune haemolysis in the dog: relationship between anemia and the levels of red blood cell immunoglobulins and complement measured by enzyme-linked antiglobulin test. Vet Immunol Immunopathol 1992:34(1-2):1-20.
8. Barker RN、Gruffydd-Jones TJ、Stokes CR 等。犬隻自體免疫溶血:貧血與紅血球免疫球蛋白及補體水平之關聯性(透過酵素連結抗球蛋白試驗測定)。獸醫免疫學與免疫病理學 1992;34(1-2):1-20。
9. Schalm OW. Autoimmune hemolytic anemia in the dog. Canine Pract 1975;2:37-45.
9. Schalm OW。犬隻自體免疫溶血性貧血。犬科臨床實踐 1975;2:37-45。
10. Stokol T, Blue JT, French TW. Idiopathic pure red cell aplasia and nonregenerative immune-mediated anemia in dogs: 43 cases (1988-1999). J Am Vet Med Assoc 2000;216(9):1429-1436.
10. Stokol T、Blue JT、French TW。犬隻特發性純紅血球再生不良與非再生性免疫介導貧血:43 例病例分析(1988-1999)。美國獸醫學會雜誌 2000;216(9):1429-1436。
11. McManus PM, Craig LE. Correlation between leukocytosis and necropsy findings in dogs with immune-mediated hemolytic anemia: 34 cases (1994-1999). J Am Vet Med Assoc 2001;218(8):1308-1313.
11. McManus PM、Craig LE。免疫介導溶血性貧血犬隻白血球增多與屍檢結果之相關性:34 例病例分析(1994-1999)。美國獸醫學會雜誌 2001;218(8):1308-1313。
12. Carr AP, Panciera DL, Kidd L. Prognostic factors for mortality and thromboembolism in canine immune-mediated hemolytic anemia: a retrospective study of 72 dogs. J Vet Intern Med 2002;16(5):504-509.
12. Carr AP、Panciera DL、Kidd L。犬隻免疫介導性溶血性貧血的死亡率與血栓栓塞預後因子:72 隻犬的回顧性研究。《獸醫內科醫學期刊》2002;16(5):504-509。
13. Burgess K, Moore A, Rand W, et al. Treatment of immune-mediated hemolytic anemia in dogs with cyclophosphamide. J Vet Intern Med 2000;14(4):456-462.
13. Burgess K、Moore A、Rand W 等。使用環磷醯胺治療犬隻免疫介導性溶血性貧血。《獸醫內科醫學期刊》2000;14(4):456-462。
14. Weinkle TK, Center SA, Randolph JF, et al. Evaluation of prognostic factors, survival rates, and treatment protocols for immune-mediated hemolytic anemia in dogs: 151 cases (1993-2002). J Am Vet Med Assoc 2005;226(11):1869-1880.
14. Weinkle TK、Center SA、Randolph JF 等。犬隻免疫介導性溶血性貧血預後因子、存活率與治療方案評估:151 例病例分析(1993-2002)。《美國獸醫學會期刊》2005;226(11):1869-1880。
15. Miller E. Immune-mediated hemolytic anemia. In: Kirk's current veterinary therapy XIV. St. Louis, Mo: Saunders Elsevier, 2009;266-271.
15. Miller E。免疫介導性溶血性貧血。收錄於:《Kirk 當代獸醫治療第十四版》。密蘇里州聖路易斯:Saunders Elsevier 出版社,2009;266-271。
16. Jackson ML, Kruth SA. Immune-mediated hemolytic anemia and thrombocytopenia in the dog: a retrospective study of 55 cases from 1979 through 1983 at the Western College of Veterinary Medicine. Can Vet J 1985;26(8):245-250.
16. Jackson ML, Kruth SA. 犬隻免疫介導性溶血性貧血與血小板減少症:1979 至 1983 年間於西方獸醫學院 55 例回溯性研究。加拿大獸醫期刊 1985;26(8):245-250.
17. Morley P, Mathes M, Guth A, et al. Anti-erythrocyte antibodies and disease associations in anemic and nonanemic dogs. J Vet Intern Med 2008;22(4):886-892.
17. Morley P, Mathes M, Guth A, 等. 貧血與非貧血犬隻之抗紅血球抗體與疾病關聯性。獸醫內科醫學期刊 2008;22(4):886-892.
18. Boozer L, Macintire D. Babesia gibsoni: An emerging pathogen in dogs. Compend Contin Educ Pract Vet 2005;27(1):33-41.
18. Boozer L, Macintire D. 犬隻新興病原體:吉布松巴貝斯蟲。獸醫臨床繼續教育彙編 2005;27(1):33-41.
19. Macintire DK, Boudreaux MK, West GD, et al. Babesia gibsoni infection among dogs in the southeastern United States. J Am Vet Med Assoc 2002;220(3):325-329.
19. Macintire DK, Boudreaux MK, West GD, 等. 美國東南部犬隻吉布松巴貝斯蟲感染狀況。美國獸醫學會期刊 2002;220(3):325-329.
20. Stegeman JR, Birkenheuer AJ, Kruger JM, et al. Transfusion-associated Babesia gibsoni infection in a dog. J Am Vet Med Assoc 2003;222(7):959-963.
20. Stegeman JR、Birkenheuer AJ、Kruger JM 等。犬隻輸血相關吉布松巴貝斯蟲感染。美國獸醫學會雜誌 2003;222(7):959-963。
21. Birkenheuer AJ, Correa MT, Levy MG, et al. Geographic distribution of babesiosis among dogs in the United States and association with dog bites: 150 cases (2000-2003). J Am Vet Med Assoc 2005;227(6):942-947.
21. Birkenheuer AJ、Correa MT、Levy MG 等。美國犬隻巴貝斯蟲病地理分佈與犬咬傷之關聯性:150 例病例分析(2000-2003)。美國獸醫學會雜誌 2005;227(6):942-947。
22. Neer MN. Ehrlichiosis. In: Greene CE, ed. Infectious diseases of the dog and cat. 2nd ed. Philadelphia, Pa: WB Saunders, 1998;139-147.
22. Neer MN。艾利希體症。收錄於:Greene CE 編。犬貓傳染病學。第 2 版。賓州費城:WB Saunders,1998;139-147。
23. Strickland KN. Canine and feline caval syndrome. Clin Tech Small Anim Pract 1998;13(2):88-95.
23. Strickland KN。犬貓腔靜脈症候群。小動物臨床技術實務 1998;13(2):88-95。
24. McCullough S. Immune-mediated hemolytic anemia: understanding the nemesis. Vet Clin North Am Small Anim Pract 2003;33(6):1295-1315.
24. McCullough S. 免疫介導性溶血性貧血:理解這個宿敵。《北美小動物臨床診療》2003;33(6):1295-1315.
25. Scott-Moncrieff JC, Treadwell NG, McCullough SM, et al. Hemostatic abnormalities with primary immune-mediated hemolytic anemia. J Am Anim Hosp Assoc 2001;37(3):220-227.
25. Scott-Moncrieff JC、Treadwell NG、McCullough SM 等。原發性免疫介導性溶血性貧血的止血異常。《美國動物醫院協會雜誌》2001;37(3):220-227.
26. Day MJ. Systemic lupus erythematosus. In: Feldman BF, Zinkl JG, Jain NC, eds. Schalm's veterinary hematology. 5th ed. Philadelphia, Pa: Lippincott, Williams & Wilkins, 2000;819-826.
26. Day MJ。系統性紅斑狼瘡。載於:Feldman BF、Zinkl JG、Jain NC 編。《Schalm 氏獸醫血液學》第 5 版。賓州費城:Lippincott, Williams & Wilkins,2000;819-826.
27. Scott-Moncrieff JC. Immune-mediated hemolytic anemia: Treatment. In: IMHA: New perspectives on a challenging disease. Thomson Veterinary Healthcare Communications, Lenexa, Kan, 2002:7-11. In: Vet Med 97(10). Sponsored insert.
27. Scott-Moncrieff JC。免疫介導性溶血性貧血:治療。載於:《IMHA:一個具挑戰性疾病的新觀點》。堪薩斯州 Lenexa:Thomson Veterinary Healthcare Communications,2002:7-11. 載於:《獸醫醫學》97(10)。贊助增刊。
28. Reimer ME, Troy GC, Warnick LD. Immune-mediated hemolytic anemia: 70 cases (1988-1996). J Am Anim Hosp Assoc 1999;35(5):384-391.
28. Reimer ME、Troy GC、Warnick LD。《免疫介導性溶血性貧血:70 例病例分析(1988-1996 年)》。美國動物醫院協會雜誌 1999;35(5):384-391。
29. Grundy SA, Barton C. Influence of drug treatment on survival of dogs with immune-mediated hemolytic anemia: 88 cases (1989-1999). J Am Vet Med Assoc 2001;218(4):543-546.
29. Grundy SA、Barton C。《藥物治療對免疫介導性溶血性貧血犬隻存活率的影響:88 例病例分析(1989-1999 年)》。美國獸醫學會雜誌 2001;218(4):543-546。
30. Mason N, Duval D, Shofer FS, et al. Cyclophosphamide exerts no beneficial effect over prednisone alone in the initial treatment of acute immune-mediated hemolytic anemia in dogs: a randomized controlled clinical trial. J Vet Intern Med 2003;17(2):206-212.
30. Mason N、Duval D、Shofer FS 等。《環磷醯胺在犬隻急性免疫介導性溶血性貧血初始治療中未顯示優於單獨使用 prednisone:隨機對照臨床試驗》。獸醫內科醫學雜誌 2003;17(2):206-212。
31. Gregory CR. Immunosuppressive agents. In: Kirk's current veterinary therapy XIII small animal practice. Philadelphia, Pa: WB Saunders Co, 2000;509-513.
31. Gregory CR。《免疫抑制劑》。載於:Kirk 當代獸醫治療學第十三版小動物臨床手冊。賓州費城:WB Saunders 出版社,2000 年;509-513 頁。
32. Nielsen L, Niessen S, Ramsay IK, et al. The use of mycophenolate mofetil in eight dogs with idiopathic immune mediated haemolytic anaemia, in Proceedings. European Coll Vet Intern Med Companion Anim Congress 2005.
32. Nielsen L、Niessen S、Ramsay IK 等。黴酚酸酯在八隻特發性免疫介導溶血性貧血犬隻的應用,見《歐洲獸醫內科醫學會伴侶動物大會論文集》2005 年。
33. Miller E. The use of danazol in the therapy of immune-mediated disease of dogs. Semin Vet Med Surg (Small Anim) 1997;12(3):167-169.
33. Miller E。丹那唑在犬隻免疫介導疾病治療中的應用。《小動物獸醫內外科研討會》1997 年;12(3):167-169。
34. White HL, O'Toole TE, Rozanski EA, et al. Early treatment of canine immune-mediated hemolytic anemia with intravenous immunoglobulin: 11 cases (1998-2001) (abst). J Vet Intern Med 2002;16(3):318.
34. White HL、O'Toole TE、Rozanski EA 等。靜脈注射免疫球蛋白早期治療犬免疫介導溶血性貧血:11 例報告(1998-2001 年)(摘要)。《獸醫內科醫學期刊》2002 年;16(3):318。
35. Mathes M, Jordan M, Dow S. Evaluation of liposomal clodronate in experimental spontaneous autoimmune hemolytic anemia in dogs. Exp Hematol 2006;34(10):1393-1402.
35. Mathes M、Jordan M、Dow S。脂質體氯膦酸鹽在犬自發性自體免疫溶血性貧血實驗中的評估。《實驗血液學》2006 年;34(10):1393-1402。
36. Lunn KF. Liposomal clodronate as a novel treatment for immune-mediated hemolytic anemia in dogs. Clinical Trials and Research Projects, Colorado State University, Fort Collins, CO. Personal communication, October 2008.
36. Lunn KF。脂質體氯膦酸鹽作為犬隻免疫介導性溶血性貧血的新型治療方法。臨床試驗與研究項目,科羅拉多州立大學,科林斯堡,科羅拉多州。個人通訊,2008 年 10 月。
37. Toll, J, Aronsohn M. Prospective evaluation of medical therapy with or without early splenectomy for treatment of severe immune-mediated hemolytic anemia in the dog, in Proceedings, Am Coll Vet Intern Med 2003.
37. Toll, J, Aronsohn M。針對犬隻嚴重免疫介導性溶血性貧血,早期脾切除術合併藥物治療之前瞻性評估,刊載於《美國獸醫內科醫學會會議論文集》2003 年。
38. Thompson MF, Scott-Moncreiff JC, Brooks MB. Effect of a single plasma transfusion on thromboembolism in 13 dogs with primary immune-mediated hemolytic anemia. J Am Anim Hosp Assoc 2004;40(6):446-454.
38. Thompson MF, Scott-Moncreiff JC, Brooks MB。單次血漿輸注對 13 隻原發性免疫介導性溶血性貧血犬隻血栓栓塞之影響。《美國動物醫院協會雜誌》2004;40(6):446-454。
39. Breuhl EL, Scott-Moncrieff C, Brooks M. A prospective study of unfractionated heparin therapy to prevent thrombosis in canine immune-mediated hemolytic anemia, in Proceedings. Am Coll Vet Intern Med 2005.
39. Breuhl EL, Scott-Moncrieff C, Brooks M。未分餾肝素治療預防犬隻免疫介導性溶血性貧血血栓形成之前瞻性研究,刊載於《美國獸醫內科醫學會會議論文集》2005 年。
40. Birkenheuer AJ, Le JA, Valenzisi AM, et al. Cytauxzoon felis infection in cats in the mid-Atlantic states: 34 cases (1998-2004). J Am Vet Med Assoc 2006;228(4):568-571.
40. Birkenheuer AJ、Le JA、Valenzisi AM 等。中大西洋各州貓隻感染 Cytauxzoon felis:34 例病例報告(1998-2004)。《美國獸醫學會雜誌》2006;228(4):568-571。
41. Kohn B, Weingart C, Eckmann V, et al. Primary immune-mediated hemolytic anemia in 19 cats: diagnosis, therapy, and outcome (1998-2004). J Vet Intern Med 2006;20(1):159-166.
41. Kohn B、Weingart C、Eckmann V 等。19 例貓原發性免疫介導溶血性貧血:診斷、治療與預後(1998-2004)。《獸醫內科醫學雜誌》2006;20(1):159-166。
42. de Brito Galvao JF, Trepanier LA. Risk of hemolytic anemia with intravenous administration of famotidine to hospitalized cats. J Vet Intern Med 2008;22(2):325-329.
42. de Brito Galvao JF、Trepanier LA。住院貓靜脈注射法莫替丁引發溶血性貧血風險。《獸醫內科醫學雜誌》2008;22(2):325-329。
43. Noble SJ, Armstrong PJ. Bee sting envenomation in secondary immune-mediated hemolytic anemia in two dogs. J Am Vet Med Assoc 1999;214(7):1026-1027.
43. Noble SJ、Armstrong PJ。兩例犬隻繼發性免疫介導溶血性貧血合併蜂螫中毒。《美國獸醫學會雜誌》1999;214(7):1026-1027。
44. Trepanier L. Idiosyncratic toxicity associated with potentiated sulfonamides in the dog. J Vet Pharmacol Ther 2004:27(3):129-138.
44. Trepanier L. 犬隻對增效磺胺類藥物的特異性毒性反應。《獸醫藥理學與治療學期刊》2004 年;27(3):129-138。
45. Bloom JC, Thiem PA, Sellers TS, et al. Cephalosporin-induced immune mediated cytopenia in the dog: demonstration of erythrocyte-, neutrophil-, and platelet- associated IgG following treatment with cefazedone. Am J Hematol 1988:28(2):71-78.
45. Bloom JC、Thiem PA、Sellers TS 等。頭孢菌素誘發犬隻免疫媒介性血球減少症:使用頭孢西酮治療後紅血球、嗜中性球及血小板相關 IgG 之證實。《美國血液學期刊》1988 年;28(2):71-78。
46. Peterson M. Hyperthyroidism. In: Ettinger SJ, Feldman EC, eds. Textbook of veterinary internal medicine. 5th ed. St. Louis, Mo: Elsevier Co, 2000;1410-1411.
46. Peterson M. 甲狀腺功能亢進。收錄於:Ettinger SJ、Feldman EC 編。《獸醫內科學教科書》第 5 版。密蘇里州聖路易斯:Elsevier 公司,2000 年;1410-1411 頁。
47. EC Feldman, RW Nelson. Feline hyperthyroidism (thyrotoxicosis). Canine and feline endocrinology and reproduction. 3rd ed. St. Louis, Mo: Elsevier Co, 2004;152-218.
47. EC Feldman、RW Nelson。貓甲狀腺功能亢進症(甲狀腺毒症)。《犬貓內分泌學與生殖學》第 3 版。密蘇里州聖路易斯:Elsevier 公司,2004 年;152-218 頁。
48. Bexfield NH, Villiers EJ, Herrtage ME. Immune-mediated haemolytic anemia and thrombocytopenia associated with Anaplasma phagocytophilum in a dog. J Small Anim Pract 2005;46(11):543-548.
48. Bexfield NH、Villiers EJ、Herrtage ME。《與犬隻嗜吞噬細胞無形體感染相關之免疫媒介性溶血性貧血及血小板減少症》。J Small Anim Pract 2005;46(11):543-548。
Newsletter 電子報
From exam room tips to practice management insights, get trusted veterinary news delivered straight to your inbox—subscribe to dvm360.
從診間技巧到診所管理洞見,獲取值得信賴的獸醫資訊直接送達您的收件匣—訂閱 dvm360

角膜潰瘍:常見誤解
角膜潰瘍治療指南:藥物管理與清創術的抉擇
瞭解犬隻患者的移行細胞癌
Janus 激酶抑制劑的效果如何?
克服診斷和治療貓過敏的挑戰
鱗狀細胞癌治療與管理的最新進展
診斷貓咪患者的慢性腎臟病
新生兒復甦的最佳實踐
為什麼犬隻骨關節炎如此複雜?
如何有效管理犬隻骨關節炎
Practical weight loss in cats
貓咪實用減重指南
With these practical tips for cat weight loss, we can empower clients to help their cats have normal body condition, while maintaining if not improving the human animal bond
透過這些實用的貓咪減重建議,我們能幫助飼主協助愛貓恢復標準體態,同時維持甚至增進人寵之間的情感連結
Read More 閱讀更多
Eye to eye: Navigating ophthalmology emergencies
眼對眼:眼科急症的診療導航
Alex Sigmund, DVM, DACVO, shares his expertise on dealing with ocular emergencies on this episode of The Vet Blast Podcast presented by dvm360.
Alex Sigmund 獸醫學博士、美國獸醫眼科專科醫師(DACVO)在本期由 dvm360 製作的《獸醫快訊播客》中分享他處理眼科急症的專業見解。
Listen 收聽
Get in the know with Lepto
認識鉤端螺旋體病
Christopher Lee, DVM, MPH, DACVPM, provides listeners with more information on Leptospirosis, including whether or not vaccinations are dangerous for patients.
Christopher Lee 獸醫師,公共衛生碩士,美國預防獸醫學院認證醫師,為聽眾提供更多關於鉤端螺旋體病的資訊,包括疫苗接種對病患是否具有危險性。
Read More 閱讀更多
Case study: Linear foreign body in feline patients
病例研究:貓病患的線性異物
Objects can get caught around the base of the tongue, knot up in the stomach, and become lodged in the pylorus or further down in the gastrointestinal tract
異物可能卡在舌根處、在胃中打結,或是卡在幽門或更下方的胃腸道中
Read More 閱讀更多





