 Tianzhichao Hou Tianzhichichao Hou1,2†
Tianzhichao Hou Tianzhichichao Hou1,2† Huajie Dai 戴华杰1,2†
Huajie Dai 戴华杰1,2† Qi Wang 王琦1,2†
Qi Wang 王琦1,2† Yanan Hou 延安侯1,2
Yanan Hou 延安侯1,2 Xiaoyun Zhang 张晓云1,2
Xiaoyun Zhang 张晓云1,2 Hong Lin 林虹1,2
Hong Lin 林虹1,2 Shuangyuan Wang 王双元1,2
Shuangyuan Wang 王双元1,2 Mian Li 李勉1,2
Mian Li 李勉1,2 Zhiyun Zhao 赵志云1,2
Zhiyun Zhao 赵志云1,2 Jieli Lu1,2
Jieli Lu1,2 Yu Xu 余旭1,2
Yu Xu 余旭1,2 Yuhong Chen 陈玉红1,2
Yuhong Chen 陈玉红1,2 Yanyun Gu 顾燕云1,2
Yanyun Gu 顾燕云1,2 Jie Zheng1,2
Jie Zheng1,2 Tiange Wang 王天戈1,2
Tiange Wang 王天戈1,2 Weiqing Wang 王伟清1,2
Weiqing Wang 王伟清1,2 Yufang Bi 毕玉芳1,2Guang Ning 广宁1,2
Yufang Bi 毕玉芳1,2Guang Ning 广宁1,2 Min Xu 徐敏1,2*
Min Xu 徐敏1,2*- 1Department of Endocrine and Metabolic Diseases, Shanghai Institute of Endocrine and Metabolic Diseases, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
1 上海交通大学医学院附属瑞金医院上海内分泌与代谢病研究所内分泌与代谢病科,中国上海 - 2Shanghai National Clinical Research Center for Metabolic Diseases, Key Laboratory for Endocrine and Metabolic Diseases of the National Health Commission of the PR China, Shanghai Key Laboratory for Endocrine Tumor, State Key Laboratory of Medical Genomics, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
2 上海国家代谢病临床医学研究中心、国家卫生健康委员会内分泌与代谢病重点实验室、上海市内分泌肿瘤重点实验室、医学基因组学国家重点实验室、上海交通大学医学院附属瑞金医院,中国上海
Objectives: Our aim was to investigate the interactive causal effects between gut microbiota and host urate metabolism and explore the underlying mechanism using genetic methods.
研究目的我们的目的是研究肠道微生物群与宿主尿酸盐代谢之间的交互因果效应,并利用遗传学方法探索其潜在机制。
Methods: We extracted summary statistics from the abundance of 211 microbiota taxa from the MiBioGen (N =18,340), 205 microbiota metabolism pathways from the Dutch Microbiome Project (N =7738), gout from the Global Biobank Meta-analysis Initiative (N =1,448,128), urate from CKDGen (N =288,649), and replication datasets from the Global Urate Genetics Consortium (N gout =69,374; N urate =110,347). We used linkage disequilibrium score regression and bidirectional Mendelian randomization (MR) to detect genetic causality between microbiota and gout/urate. Mediation MR and colocalization were performed to investigate potential mediators in the association between microbiota and urate metabolism.
方法:我们从 MiBioGen 的 211 个微生物群分类群(N =18,340 个)、荷兰微生物组项目(N =7738 个)的 205 个微生物群代谢途径、全球生物库元分析倡议(Global Biobank Meta-analysis Initiative)的痛风(N =1,448,128 个)、CKDGen 的尿酸盐(N =288,649 个)以及全球尿酸盐遗传学联合会(Global Urate Genetics Consortium)的复制数据集(N gout =69,374;N urate =110,347)。我们使用连锁不平衡得分回归和双向孟德尔随机化(MR)来检测微生物群与痛风/尿酸之间的遗传因果关系。为了研究微生物群与尿酸盐代谢之间关系的潜在中介因素,我们进行了中介MR和共定位。
Results: Two taxa had a common causal effect on both gout and urate, whereas the Victivallaceae family was replicable. Six taxa were commonly affected by both gout and urate, whereas the Ruminococcus gnavus group genus was replicable. Genetic correlation supported significant results in MR. Two microbiota metabolic pathways were commonly affected by gout and urate. Mediation analysis indicated that the Bifidobacteriales order and Bifidobacteriaceae family had protective effects on urate mediated by increasing docosahexaenoic acid. These two bacteria shared a common causal variant rs182549 with both docosahexaenoic acid and urate, which was located within MCM6/LCT locus.
结果有两个类群对痛风和尿酸盐都有共同的致病作用,而维克瓦伦科(Victivallaceae)类群具有可复制性。6 个类群对痛风和尿酸盐均有共同影响,而 Ruminococcus gnavus 群属具有可复制性。遗传相关性支持 MR 的重要结果。痛风和尿酸盐通常会影响两个微生物群的代谢途径。中介分析表明,双歧杆菌目和双歧杆菌科通过增加二十二碳六烯酸对尿酸盐具有保护作用。这两种细菌与二十二碳六烯酸和尿酸盐共享一个共同的因果变异体 rs182549,该变异体位于 MCM6/LCT 基因座内。
Conclusions: Gut microbiota and host urate metabolism had a bidirectional causal association, implicating the critical role of host-microbiota crosstalk in hyperuricemic patients. Changes in gut microbiota can not only ameliorate host urate metabolism but also become a foreboding indicator of urate metabolic diseases.
结论肠道微生物群与宿主尿酸盐代谢之间存在双向因果关系,这表明宿主-微生物群之间的串联在高尿酸血症患者中发挥着关键作用。肠道微生物群的变化不仅能改善宿主的尿酸盐代谢,还能成为尿酸盐代谢疾病的预兆指标。
1 Introduction 1 引言
Gout is a prevalent inflammatory condition characterized by a sustained high serum urate concentration and intermittent episodes of severely painful arthritis (gout flares) (1). It is the second most common metabolic disease after type 2 diabetes and leads to an increased rate of subsequent cardiovascular complications (2). Epidemiological investigations showed gout prevalence ranging from <1% to 6.8% worldwide, which was highly related to patients’ genetics, lifestyles, and social and economic status (3). Recently, gut microbiota was reported to be associated with the pathogenesis of hyperuricemia. The abundance and composition changes in gut microbiota might increase serum uric acid levels through the dysfunction of uric acid degradation and increased uric acid production (4). Meanwhile, gut microbiota also plays a crucial role in treating metabolic diseases using probiotics and prebiotics (5, 6). Therefore, the human microbiota is gradually recognized as a novel target for a better understanding of the pathogenesis of gout and hyperuricemia.
痛风是一种常见的炎症,其特点是血清尿酸盐浓度持续偏高,间歇性发作剧烈疼痛的关节炎(痛风发作) ( 1)。痛风是仅次于 2 型糖尿病的第二大常见代谢性疾病,并导致后续心血管并发症的发生率增加 ( 2)。流行病学调查显示,痛风在全球的发病率从<1%到6.8%不等,与患者的遗传、生活方式、社会和经济状况有很大关系(3)。最近,有报道称肠道微生物群与高尿酸血症的发病机制有关。肠道微生物群的丰度和组成变化可能会通过尿酸降解功能障碍和尿酸生成增加而增加血清尿酸水平(4)。同时,肠道微生物群在利用益生菌和益生元治疗代谢性疾病方面也起着至关重要的作用(5,6)。因此,人类微生物群逐渐被认为是更好地了解痛风和高尿酸血症发病机制的新靶点。
However, previous studies focusing on the bacteria-urate interplay faced several obstacles, including inadequate participants, cross-sectional design, and less evidence of causality, as well as the fact that most of the studies were conducted within the Asian population (7–10). In addition, the underlying mechanism linking gut bacteria with urate metabolism has not been well established. Gut microbiota and its metabolites were associated with rheumatic diseases including gout, rheumatoid arthritis, and osteoarthritis via fatty acids (11). An experimental study investigated the impact of polyunsaturated fatty acids (PUFAs) in the handling of urate by inhibiting urate transporters in vitro (12). Some observational studies also suggested that ω-3 PUFAs, especially DHA were highly related to hyperuricemia (13, 14). However, a recent clinical trial found no significant difference in the serum urate level between the 24-week ω-3 PUFAs supplement group and the control group (15). Since gut microbiota might confer an effect on the host health status by metabolizing PUFAs (16), we hereby hypothesize a potential mediation effect of gut microbiota on urate metabolism via PUFAs and their important subtypes, such as DHA.
然而,以往关注细菌与尿酸盐相互作用的研究面临着一些障碍,包括参与者不足、横断面设计、因果关系证据较少,以及大多数研究都是在亚洲人群中进行的(7-10)。此外,肠道细菌与尿酸盐代谢之间的内在机制尚未得到很好的证实。肠道微生物群及其代谢产物通过脂肪酸与痛风、类风湿性关节炎和骨关节炎等风湿性疾病有关(11)。一项实验研究调查了多不饱和脂肪酸(PUFAs)通过抑制体外尿酸盐转运体对尿酸盐处理的影响(12)。一些观察性研究也表明,ω-3 多不饱和脂肪酸,尤其是 DHA 与高尿酸血症密切相关 ( 13, 14)。然而,最近的一项临床试验发现,补充ω-3 PUFAs 24 周组与对照组的血清尿酸水平无明显差异(15)。由于肠道微生物群可能通过代谢 PUFAs(16)对宿主的健康状况产生影响,我们在此假设肠道微生物群通过 PUFAs 及其重要亚型(如 DHA)对尿酸盐代谢产生潜在的调节作用。
Given the ambiguous connection between gut bacteria and urate metabolism, we used several genetic methods to investigate the bidirectional causal effects between gut microbiota and urate metabolism and further explored potential mediators. Lifelong exposure to genetic methods could draw stable conclusions about the association and provide more evidence for probiotics treatment on urate metabolic disorders.
鉴于肠道细菌与尿酸盐代谢之间的联系不明确,我们采用了多种遗传学方法来研究肠道微生物群与尿酸盐代谢之间的双向因果效应,并进一步探索潜在的中介因素。长期接触遗传学方法可得出稳定的关联结论,并为益生菌治疗尿酸盐代谢紊乱提供更多证据。
2 Methods 2 种方法
2.1 Study design 2.1 研究设计
Firstly, we extracted summary statistics of gut microbiota, microbiota metabolism pathways, gout, urate level, and docosahexaenoic acid percentage (DHA, a kind of polyunsaturated fatty acid previously mentioned in clinical trials) from the respective consortiums. Secondly, we performed a large-scale bidirectional Mendelian randomization (MR) and bivariate linkage disequilibrium score regression (LDSC) to explore the genetic causality and correlation between microbiota phenotypes (gut microbiota abundance and microbiota metabolism pathways) and urate phenotypes (host gout and urate level). Finally, we used mediation analysis and colocalization to investigate the interaction of gut microbiota, DHA percentage, and urate metabolism (Figure 1). The MR analysis was reported as per the STROBE-MR guidelines, and we adopted several methods to follow the three fundamental assumptions of MR (Table S1) (17).
首先,我们从各联盟中提取了肠道微生物群、微生物群代谢途径、痛风、尿酸水平和二十二碳六烯酸百分比(DHA,临床试验中提到的一种多不饱和脂肪酸)的汇总统计数据。其次,我们进行了大规模双向孟德尔随机化(MR)和双变量联系不平衡得分回归(LDSC),以探讨微生物群表型(肠道微生物群丰度和微生物群代谢途径)与尿酸盐表型(宿主痛风和尿酸盐水平)之间的遗传因果关系和相关性。最后,我们利用中介分析和共定位研究了肠道微生物群、DHA 百分比和尿酸盐代谢之间的相互作用(图 1)。MR分析是根据STROBE-MR指南进行报告的,我们采用了多种方法来遵循MR的三个基本假设(表S1)( 17)。
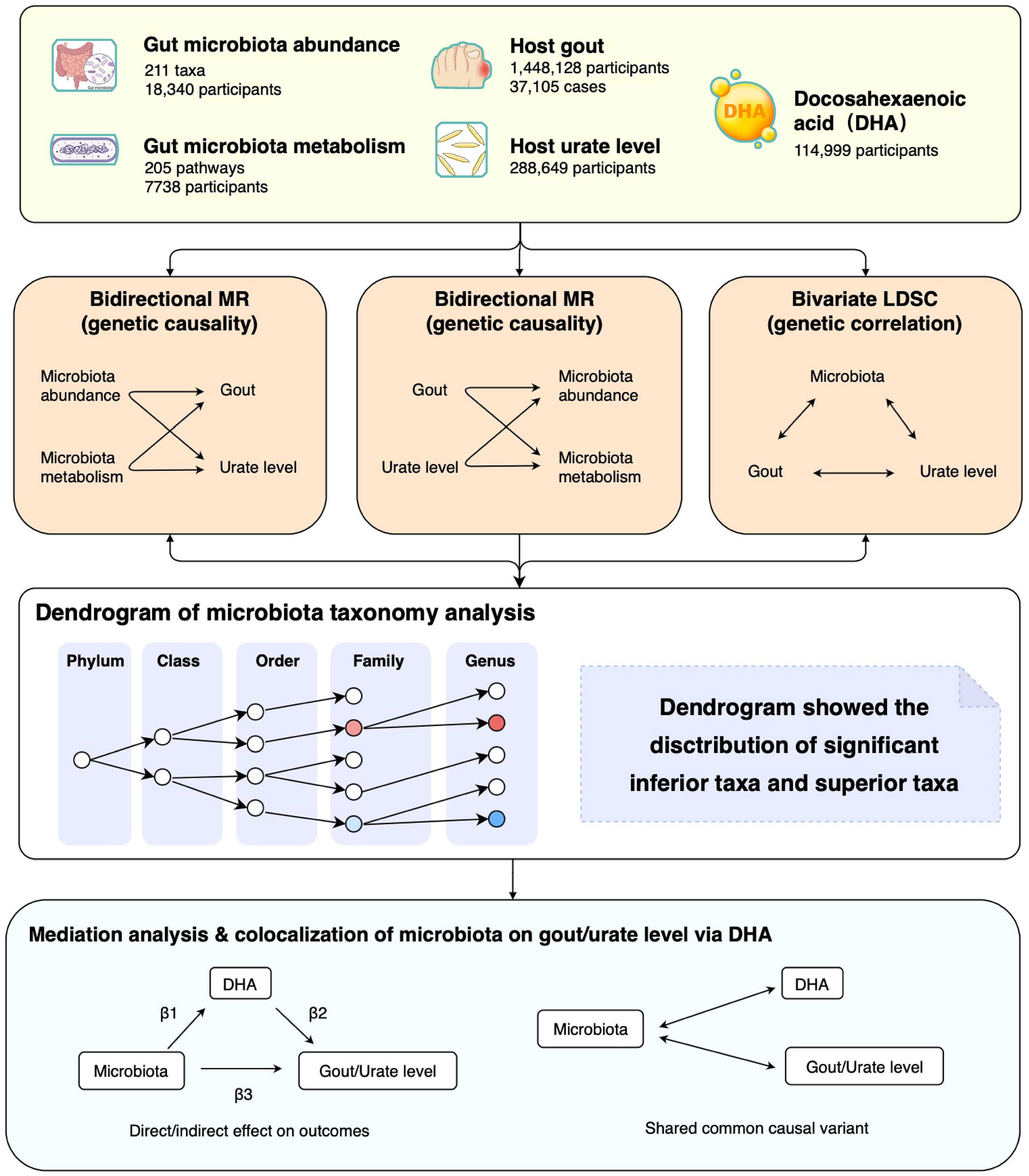
Figure 1 Study design and flowchart. MR, Mendelian randomization; LDSC, Linkage disequilibrium score regression.
图 1 研究设计和流程图。MR:孟德尔随机化;LDSC:连锁不平衡分数回归。
2.2 Instrument variables selection
2.2 工具变量的选择
Summary statistics for gut microbiota abundance were extracted from a genome-wide association study (GWAS) of host genetic variation in 18,340 multiple-ancestries participants (85% European-ancestry) from the MiBioGen consortium (Table S2) (18). It included 211 taxa: 9 phyla, 16 classes, 20 orders, 35 families, and 131 genera determined by the 16S ribosomal RNA gene sequencing. Summary statistics for microbiota metabolism pathways were extracted from the Dutch Microbiome Project (DMP) in 7738 European-ancestry participants, in which the metabolism pathways were determined by shotgun metagenomic sequencing (19). Included in the subsequent analysis were 205 bacteria metabolism pathways.
肠道微生物群丰度的简要统计数据是从 MiBioGen 联合体(表 S2)对 18,340 名多巢穴参与者(85% 为欧洲巢穴)的宿主遗传变异进行的全基因组关联研究(GWAS)中提取的(18)。它包括 211 个类群:9 个门、16 个类、20 个目、35 个科和 131 个属,由 16S 核糖体 RNA 基因测序确定。荷兰微生物组项目(Dutch Microbiome Project,DMP)从 7738 名欧洲籍参与者中提取了微生物群代谢途径的汇总统计数据,其中代谢途径是通过霰弹枪元基因组测序确定的(19)。随后的分析包括 205 条细菌代谢途径。
Summary statistics for gout were from the Global Biobank Meta-analysis Initiative (GBMI) (20). It is a collaborative network of 19 biobanks from four continents representing more than 2.1 million consenting individuals with genetic data linked to electronic health records. We used the gout data of both multi-ancestry (N = 1,448,128, 72% European-ancestry, and N cases =37,105) and European-ancestry (N = 1,069,839; N cases = 30,549). Summary statistics for urate level were from the CKDGen Consortium, including 288,649 European participants (21). We also used phenotypes of both gout (N =69,374 participants) and urate level (N =110,347 participants) from GUGC Consortium as an independent replication analysis (22). Summary statistics for blood DHA and PUFAs were from the largest GWAS for metabolites in the UK Biobank, including 114,999 European participants (23). However, the summary statistics of eicosapentaenoic acid or other specific subtypes of PUFAs were not available for this study.
痛风的汇总统计数据来自全球生物库元分析倡议(GBMI)( 20)。这是一个由来自四大洲的 19 个生物库组成的合作网络,代表了 210 多万名同意将基因数据与电子健康记录相链接的个人。我们使用了多血统(N=1,448,128,72%为欧洲血统,病例数=37,105)和欧洲血统(N=1,069,839;病例数=30,549)的痛风数据。尿酸水平的汇总统计数据来自 CKDGen Consortium,其中包括 288,649 名欧洲参与者 ( 21)。我们还使用了来自 GUGC 联合会的痛风表型(N = 69,374 名参与者)和尿酸水平表型(N = 110,347 名参与者)作为独立的复制分析 ( 22)。血液中 DHA 和 PUFAs 的汇总统计数据来自英国生物库(UK Biobank)中最大的代谢物 GWAS,包括 114999 名欧洲参与者(23)。然而,本研究没有获得二十碳五烯酸或其他特定亚型 PUFAs 的汇总统计数据。
The IV selection of exposures in bidirectional MR followed the following criteria. For each microbiota taxon and pathway, variants with genome-wide significance P <1×10−5 and effect allele frequency (EAF) >0.01 were included. All these genetic variants were clumped to a linkage disequilibrium threshold of r2 <0.001 using the 1000 Genomes European reference panel. We also calculated the F-statistics to avoid weak instrument bias. Due to the different genotyping platforms of the GWAS, some single nucleotide polymorphisms (SNPs) representing gut microbiota might be missing in the GWAS outcome, which might cause statistical bias if we simply discarded those missing SNPs. Therefore, we used proxy SNPs with LD r2 >0.8 as substitutes for these missing SNPs (24, 25). Finally, the remaining genetic variants were used as IVs to model the effect of specific taxa and pathways of gut microbiota. For gout and urate level, SNPs with genome-wide significance P <5×10−8 and EAF >0.01 were included. All SNPs were clumped to an LD threshold of r2 <0.001 using the 1000 Genomes European reference panel (26).
双向 MR 中暴露因子的 IV 选择遵循以下标准。对于每个微生物群分类群和途径,纳入全基因组显著性 P<1×10 −5 and effect allele frequency (EAF) >0.01 的变异。所有这些基因变异都被聚类到 r 2 0.8 的连锁不平衡阈值,作为缺失变异的替代。<0.001 using the 1000 Genomes European reference panel. We also calculated the F-statistics to avoid weak instrument bias. Due to the different genotyping platforms of the GWAS, some single nucleotide polymorphisms (SNPs) representing gut microbiota might be missing in the GWAS outcome, which might cause statistical bias if we simply discarded those missing SNPs. Therefore, we used proxy SNPs with LD r 2 >0.8 作为这些缺失 SNP 的替代 ( 24, 25)。最后,剩余的遗传变异作为 IV 来模拟肠道微生物群特定类群和途径的影响。对于痛风和尿酸水平,纳入了全基因组显著性 P<5×10 −8 and EAF >0.01 的 SNP。所有的 SNPs 都被聚类到 r 2 <0.001 的 LD 阈值。<0.001。
2.3 Genetic causality and correlation of microbiota and urate metabolism
2.3 微生物群与尿酸盐代谢的遗传因果关系和相关性
We obtained the MR estimates for the causal effect using the inverse-variance weighted (IVW) method (27). The estimate was provided as effect size (β) with a 95% confidence interval (CI). MR results of a specific taxon or pathway which were significant (P <0.05) in both gout and urate level with the same direction were defined as “common”. To control type 1 error, a significant taxon (P <0.05) that could be replicated in the independent GUGC cohort was defined as “replicated”; other significant MR results (P <0.05) were defined as nominally significant. Results of taxa were mapped in the dendrograms to investigate the distribution of significant inferior and superior taxa. The heterogeneity of effects was assessed by Cochran’s Q test. We performed several sensitivity analyses using the weighted median, mode-based, MRPRESSO, and contamination mixture methods to validate the results from the IVW method (28–32). We also used the MR-Steiger filtering to determine an actual causal direction. The MR-Egger intercept was used to assess the horizontal pleiotropy. Any results whose P value of Egger intercept was <0.05 were excluded.
我们使用逆方差加权法(IVW)(27)获得了因果效应的 MR 估计值。估计值以效应大小(β)和 95% 置信区间(CI)的形式提供。对痛风和尿酸水平均有显著影响(P <0.05)且方向相同的特定分类群或途径的 MR 结果被定义为 "共同"。为控制类型1错误,在独立的GUGC队列中复制的显著分类群(P<0.05)定义为 "复制";其他显著的MR结果(P<0.05)定义为名义上的显著。分类群的结果在树枝图中进行映射,以研究显著的下级分类群和上级分类群的分布情况。效应的异质性通过 Cochran's Q 检验进行评估。我们使用加权中位数、基于模式、MRPRESSO 和污染混合物方法进行了多项敏感性分析,以验证 IVW 方法的结果 ( 28- 32)。我们还使用了 MR-Steiger 滤波法来确定实际的因果方向。MR-Egger截距用于评估水平多效性。任何 Egger 截距 P 值小于 0.05 的结果都被排除在外。
We also used single-variate LDSC to estimate the heritability of 211 microbiota taxa, gout, and urate level. LD scores were calculated for all high-quality genetic variants (i.e., INFO score > 0.9 and EAF > 0.01) from each GWAS. To further understand the genetic correlation, we conducted a pair-wise genetic correlation analysis of the 211 microbiota taxa and both gout and urate level using bivariate LDSC based on the GWAS summary statistics. The genetic correlation between gout and urate level was also calculated to estimate the genetic similarity in two independent cohorts.
我们还使用单变异 LDSC 来估计 211 个微生物群分类群、痛风和尿酸水平的遗传率。我们计算了每个 GWAS 中所有高质量遗传变异的 LD 分数(即 INFO 分数 > 0.9 和 EAF > 0.01)。为了进一步了解遗传相关性,我们根据 GWAS 的汇总统计,使用双变量 LDSC 对 211 个微生物群分类群与痛风和尿酸水平进行了配对遗传相关性分析。我们还计算了痛风和尿酸水平之间的遗传相关性,以估计两个独立队列中的遗传相似性。
2.4 Mediation analysis and colocalization of microbiota, DHA, and gout/urate level
2.4 微生物群、DHA 和痛风/尿酸水平的中介分析和共定位
To estimate the effect of DHA acting on gut microbiota, we performed mediation analysis using multivariable MR. Firstly, we conducted an MR of DHA on gout and urate level. Secondly, we performed MR of 19 microbiota (significant effect on gout or urate level) on DHA (β1). Finally, we performed multivariable MR to determine the mediation effect of the DHA in bacteria on gout and urate. The multivariable Mendelian randomization (MVMR) estimated the effect of DHA on gout and urate adjusting for bacteria (β2) and the effect of bacteria on gout and urate adjusting for bacteria. To calculate the indirect mediation effect of bacteria on disease outcomes, we used the product of coefficients method as our primary method, which is the casual effect of bacteria on outcomes via DHA (β1×β2). Thus, the proportion of the total effect mediated by DHA was estimated by dividing the indirect effect by the total effect (33, 34).
为了估计 DHA 对肠道微生物群的影响,我们使用多变量 MR 进行了中介分析。首先,我们对 DHA 对痛风和尿酸水平的影响进行了 MR 分析。其次,我们将 19 个微生物群(对痛风或尿酸水平有显著影响)与 DHA(β1)进行了 MR 分析。最后,我们进行了多变量 MR,以确定细菌中的 DHA 对痛风和尿酸盐的中介效应。多变量孟德尔随机化(MVMR)估算了调整细菌后 DHA 对痛风和尿酸盐的影响(β2),以及调整细菌后细菌对痛风和尿酸盐的影响。为了计算细菌对疾病结果的间接中介效应,我们使用了系数乘积法作为主要方法,即细菌通过 DHA 对结果的偶然效应(β1×β2)。因此,将间接效应除以总效应,就可以估算出 DHA 在总效应中所占的比例 ( 33, 34)。
We then conducted colocalization analysis to test whether the significantly mediated microbiota shared a common causal variant with both DHA and gout/urate level. The posterior probability of the specific variant ( ± 5000 bp) was colocalized with summary statistics of DHA and gout/urate levels.
然后,我们进行了共定位分析,以检验显著介导的微生物群是否与 DHA 和痛风/尿酸水平共享一个共同的因果变异。将特定变体(± 5000 bp)的后验概率与 DHA 和痛风/尿酸盐水平的汇总统计进行了共定位。
All MR analyses were based on the TwoSampleMR package in R, version 4.1.2 (24); LDSC was based on LDSC software in Python, version 1.0.1 (35); the colocalization test was performed by the coloc package in R, version 5.1.0.1 (36).
所有磁共振分析均基于 R 中的 TwoSampleMR 软件包,版本为 4.1.2 ( 24);LDSC 基于 Python 中的 LDSC 软件,版本为 1.0.1 ( 35);共聚焦测试由 R 中的 coloc 软件包执行,版本为 5.1.0.1 ( 36)。
3 Results 3 项成果
For 211 taxa in the MiBioGen consortium, the genetic variants used as IVs for each taxon exposure ranged from four to 26 SNPs (median 13 SNPs; F-statistics =21). For 205 metabolism pathways in the DMP, the genetic variants ranged from one to 20 SNPs (median 11 SNPs; F-statistics =25). Additionally, we used 54 SNPs as IVs for gout in GBMI and 88 SNPs for urate level in CKDGen (Tables S3–S5).
在 MiBioGen 联盟的 211 个分类群中,用作每个分类群暴露 IV 的遗传变异从 4 个 SNPs 到 26 个 SNPs 不等(中位数为 13 个 SNPs;F-统计量为 21)。对于 DMP 中的 205 个代谢途径,遗传变异从 1 个 SNP 到 20 个 SNP 不等(中位数为 11 个 SNP;F-统计量为 25)。此外,我们在 GBMI 中使用了 54 个 SNPs 作为痛风的 IV,在 CKDGen 中使用了 88 个 SNPs 作为尿酸水平的 IV(表 S3-S5)。
3.1 Bidirectional causal association of gut microbiota and urate metabolism
3.1 肠道微生物群与尿酸盐代谢的双向因果关系
In the MR analysis, we identified 13 and 9 taxa that causally affected gout and urate level, respectively, whereas two taxa were common in both gout and urate level (Tables S6, S7). Conversely, 16 taxa were causally affected by gout and 19 taxa by urate level, whereas 6 taxa were common (Tables S8, S9).
在 MR 分析中,我们发现分别有 13 个和 9 个类群对痛风和尿酸水平有因果影响,而痛风和尿酸水平共同影响的类群有 2 个(表 S6、S7)。相反,16 个分类群对痛风有因果影响,19 个分类群对尿酸水平有因果影响,而 6 个分类群是常见的(表 S8、S9)。
In evaluating the causal effect of microbiota on gout and urate level, we found that the increase in abundance of the Lachnospiraceae ND3007 group genus commonly had a positive causal effect on both gout and urate level; the Victivallaceae family commonly had a negative causal effect on both phenotypes (Table 1). The MR-Steiger test supported the direction of significant MR estimates. Other taxa with significant causal effects on gout or urate level are shown in Figure S1. We then mapped the MR results of 203 taxa (except for eight unknown taxa) into dendrograms. According to the bacteria taxonomy, Figures 2A, B showed that genetically predicted 20 gut microbial taxa had causal effects on urate metabolism. We found that both the Bifidobacteriaceae family and its superior Bifidobacteriales order had significant causal effects on urate level (since they had the same IVs).
在评估微生物群对痛风和尿酸水平的因果效应时,我们发现 Lachnospiraceae ND3007 科属丰度的增加通常对痛风和尿酸水平都有正向因果效应;Victivallaceae 科属通常对两种表型都有负向因果效应(表 1)。MR-Steiger 检验支持显著的 MR 估计值的方向。其他对痛风或尿酸水平有显著因果效应的类群见图 S1。然后,我们将 203 个类群(8 个未知类群除外)的 MR 结果绘制成树枝图。根据细菌分类法,图 2A、B 显示,基因预测的 20 个肠道微生物类群对尿酸盐代谢有因果效应。我们发现,双歧杆菌科及其上级双歧杆菌目都对尿酸水平有显著的因果效应(因为它们具有相同的IV)。
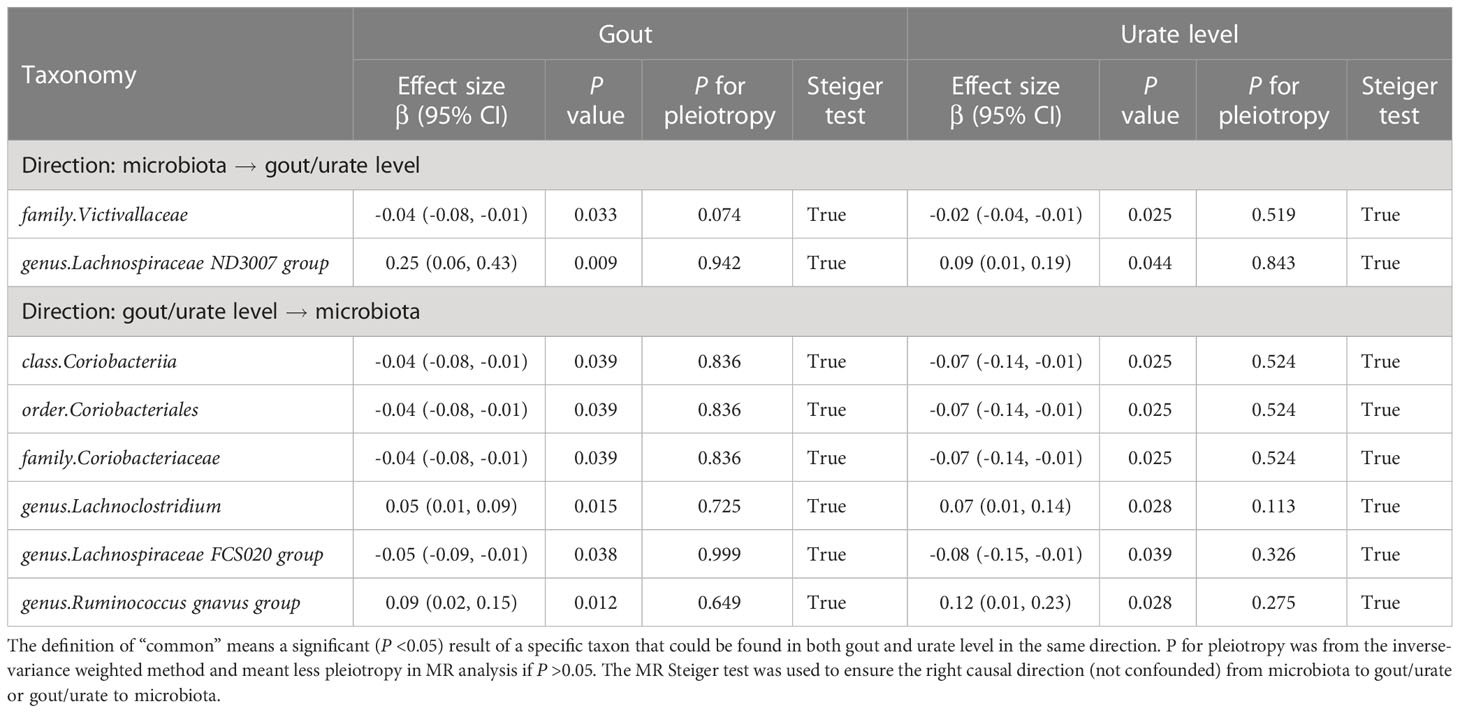
Table 1 Bidirectional MR analysis of the causal effect between gut microbiota and gout/urate level.
表 1 肠道微生物群与痛风/尿酸水平之间因果关系的双向 MR 分析。
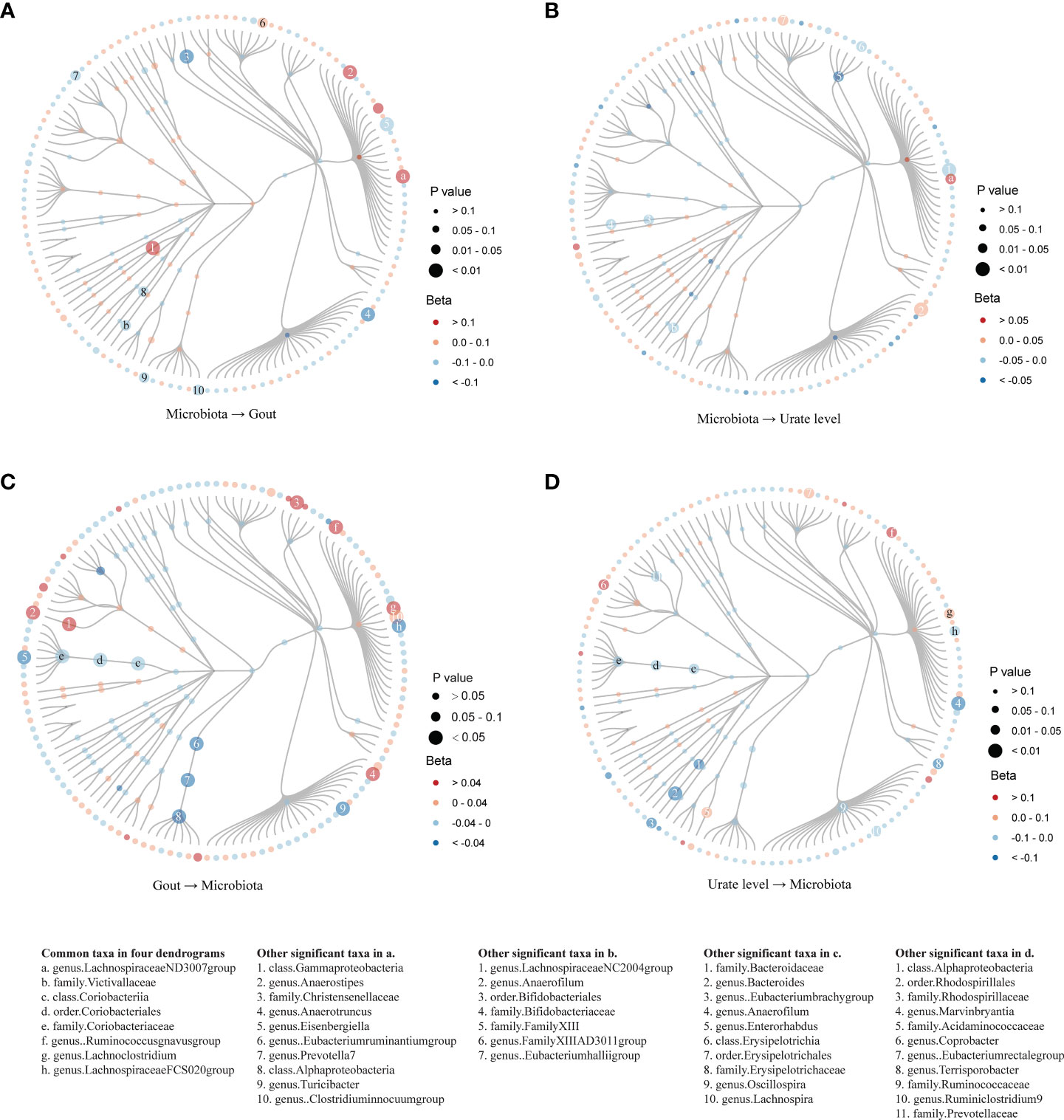
Figure 2 Dendrograms showing the taxonomy structure of the association between gut microbiota and host gout/urate level. Four dendrograms compared with the MR results of inferior and superior taxa according to the taxonomy structure. We included 203 taxa in the figures and excluded eight taxa named unknown. Taxa with significant MR results were listed at the bottom of the figure: the first column showed eight common taxa in both gout and urate level; the other four columns showed significant taxa in the respective figures. (A). MR results from microbiota to gout; (B). MR results from microbiota to urate level; (C). MR results from gout to microbiota; (D). MR results from urate level to microbiota.
图 2 显示肠道微生物群与宿主痛风/尿酸水平之间关联的分类结构的树枝图。根据分类结构比较了下级和上级类群的 MR 结果的四个树枝图。我们在图表中纳入了 203 个分类群,并排除了 8 个未知分类群。具有重要 MR 结果的类群列于图的底部:第一列显示了痛风和尿酸水平中的 8 个常见类群;其他四列显示了各自图中的重要类群。(A).从微生物群到痛风的 MR 结果;(B).从微生物群到尿酸水平的 MR 结果;(C).从痛风到微生物群的 MR 结果;(D).从尿酸水平到微生物群的 MR 结果。
In evaluating the causal effect of gout and urate level on microbiota, we found that both gout and urate level commonly had a positive causal effect on the Lachnoclostridium genus and Ruminococcus gnavus group genus; gout and urate level commonly had a negative causal effect on Coriobacteriia class, Coriobacteriales order, Coriobacteriaceae family, and Lachnospiraceae FCS020 group genus. The MR-Steiger test supported the direction of significant MR estimates (Table 1). Other taxa affected by gout or urate level such as the Bacteroides genus, Lachnoclostridium genus, and Eubacterium hallii group genus can be found in Tables S8, S9 and Figure S2. Figures 2C, D show that urate metabolism had a causal effect on 29 gut microbial taxa.
在评估痛风和尿酸水平对微生物群的因果效应时,我们发现痛风和尿酸水平通常对Lachnoclostridium属和Ruminococcus gnavus群属有正向因果效应;痛风和尿酸水平通常对Coriobacteriia类、Coriobacteriales目、Coriobacteriaceae科和Lachnospiraceae FCS020群属有负向因果效应。MR-Steiger 检验支持显著的 MR 估计值的方向(表 1)。其他受痛风或尿酸水平影响的分类群,如乳酸杆菌属、Lachnoclostridium 属和 Eubacterium hallii 组属,见表 S8、S9 和图 S2。图 2C 和 D 显示,尿酸盐代谢对 29 个肠道微生物类群有因果关系。
Finally, replicated MR analysis in the independent GUGC cohort further validated our finding. In all common taxa, the effect of the Victivallaceae family on both gout and urate level could be replicated in GUGC; the effect of both gout and urate level on the Ruminococcus gnavus group genus could also be replicated in GUGC (Table 2).
最后,在独立的 GUGC 群体中进行的重复 MR 分析进一步验证了我们的发现。在所有常见类群中,蔓荆子科对痛风和尿酸水平的影响都能在 GUGC 中得到复制;痛风和尿酸水平对瘤胃球菌属的影响也能在 GUGC 中得到复制(表 2)。
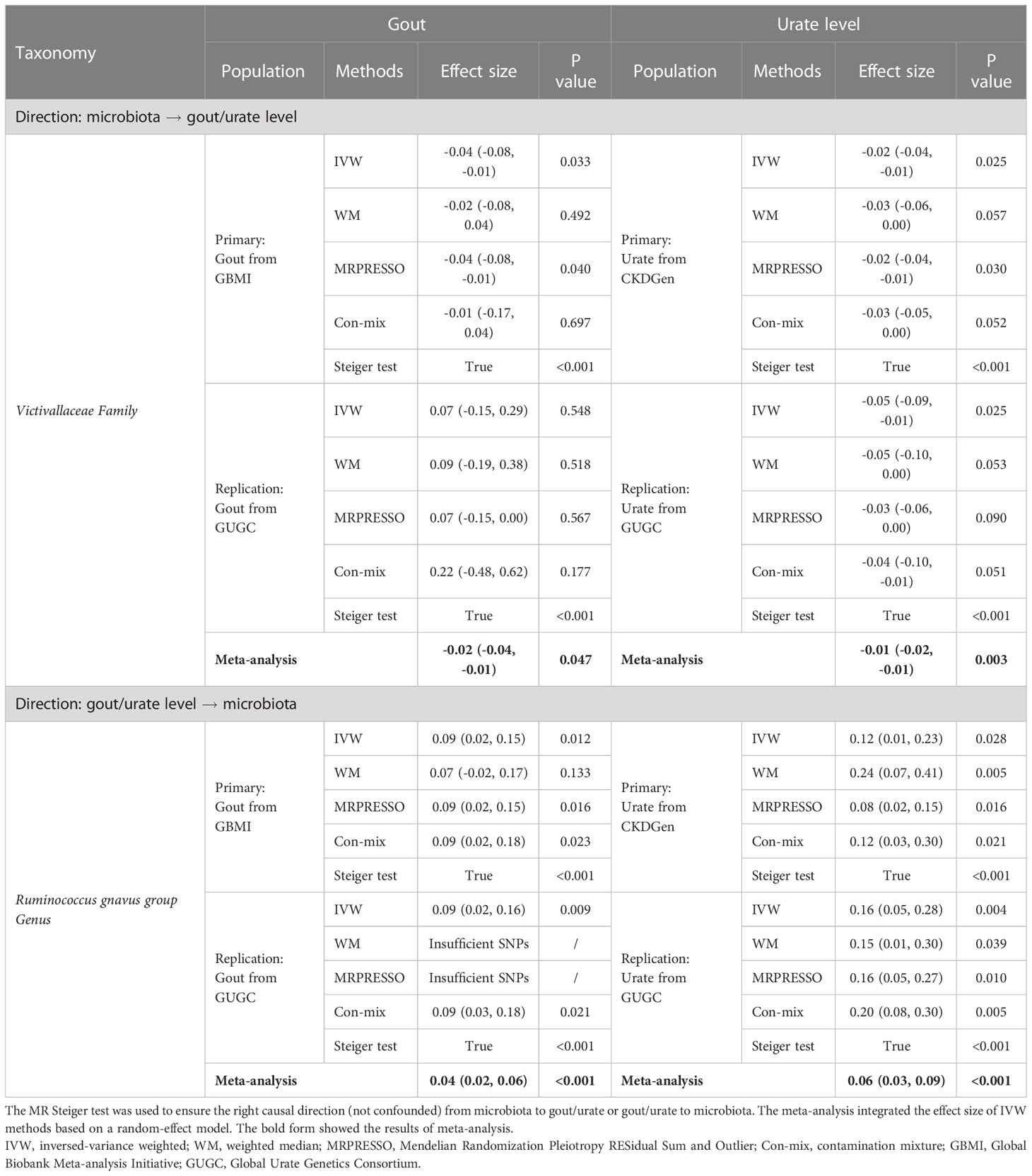
Table 2 Replicated significant taxa of bidirectional MR supported the causal effect between gut microbiota and gout/urate level.
表 2 重复的双向 MR 重要类群支持肠道微生物群与痛风/尿酸水平之间的因果效应。
Bivariate LDSC supported the genetic correlation of the Eubacteriumruminantium -group genus with gout (regression coefficient [Rg]: 0.28, P = 0.041) and the Lachnoclostridium genus with urate level (Rg: 0.28, P = 0.008), which were consistent with the MR results. Gout and urate level were highly genetically correlated (Rg: 0.89, P <0.001) (Tables S10, S11).
双变量 LDSC 支持 Eubacteriumruminantium -group 属与痛风的遗传相关性(回归系数 [Rg]:0.28,P = 0.041)和 Lachnoclostridium 属与尿酸水平的遗传相关性(Rg:0.28,P = 0.008),这与 MR 结果一致。痛风和尿酸水平在遗传上高度相关(Rg:0.89,P<0.001)(表 S10 和 S11)。
Since few significant taxa appeared in the phylum, class, and order level, we further compared the results of gout with the urate level of each taxon in the family and genus level (Figure 3). In the genus level, five genera (one was common) in the Lachnospiraceae family had a significant causal effect on either gout or urate level; gout or urate level had a significant causal effect on five genera in the Lachnospiraceae family (two were common) (Figure S3). Totally, nine genera of the Lachnospiraceae family had a significant causal association with gout or urate level, whereas the Lachnospiraceae NC2004 group genus could significantly affect host urate level and be affected by host urate level.
由于在门、纲和目水平上出现的重要类群很少,我们进一步比较了痛风与科、属水平上各类群尿酸水平的结果(图 3)。在属的水平上,漆树科的 5 个属(1 个常见属)对痛风或尿酸水平都有显著的因果关系;痛风或尿酸水平对漆树科的 5 个属(2 个常见属)都有显著的因果关系(图 S3)。总之,漆树科有 9 个属与痛风或尿酸水平有显著的因果关系,而漆树科 NC2004 属可显著影响宿主的尿酸水平,并受宿主尿酸水平的影响。
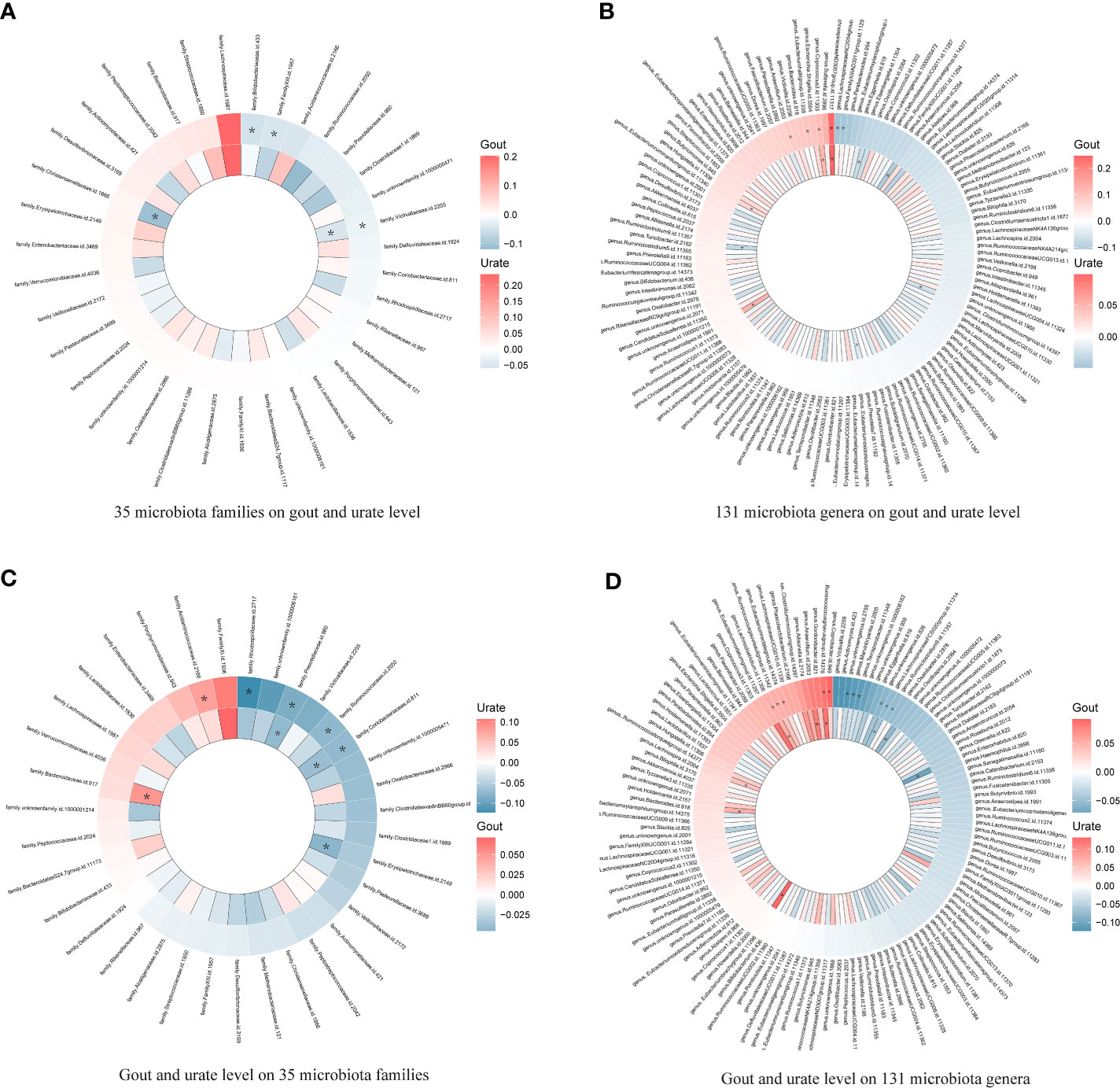
Figure 3 Heatmap showing bidirectional causality of 35 families and 131 genera. Four heatmaps comparing the results of gout with the urate level of each taxon in 35 families and 131 genera. The outer ring represents urate level and the inner ring represents gout. (A). 35 microbiota families on gout and urate level; (B). 131 microbiota genera on gout and urate level; (C). Gout and urate level on 35 microbiota families; (D). Gout and urate level on 131 microbiota genera. * means significant results.
图 3 热图显示 35 科 131 属的双向因果关系。将痛风的结果与 35 科 131 属中每个类群的尿酸水平进行比较的四张热图。外圈代表尿酸水平,内圈代表痛风。(A).35 个微生物群科与痛风和尿酸水平的关系;(B).131 个微生物群属对痛风和尿酸水平的影响;(C).痛风和尿酸水平与 35 个微生物群科的关系;(D).131 个微生物群属对痛风和尿酸水平的影响。* 表示结果有意义。
3.2 Bidirectional causal association of microbiota metabolism pathways and urate metabolism
3.2 微生物群代谢途径与尿酸盐代谢的双向因果关系
Based on the MR results (Tables S12, S13), we identified that a per unit increased abundance of eight pathways had causal effects on gout and 14 pathways had causal effects on urate level, including 1,4-dihydroxy-2-naphthoate biosynthesis (gout: β: 0.07, 95% CI: [0.01, 0.12], P = 0.014) or flavin biosynthesis (urate level: β: -0.06, 95% CI: [-0.10, -0.01], P = 0.013) (Figure 4).
根据 MR 结果(表 S12、S13),我们发现单位丰度增加的 8 个通路对痛风有因果效应,14 个通路对尿酸水平有因果效应,包括 1,4-二羟基-2-萘甲酸酯生物合成(痛风:β:0.07,95% CI:[0.01,0.12],P = 0.014)或黄素生物合成(尿酸水平:β:-0.06,95% CI:-0.06,P = 0.014)。07,95% CI:[0.01,0.12],P = 0.014)或黄素生物合成(尿酸水平:β:-0.06,95% CI:[-0.10,-0.01],P = 0.013)(图 4)。
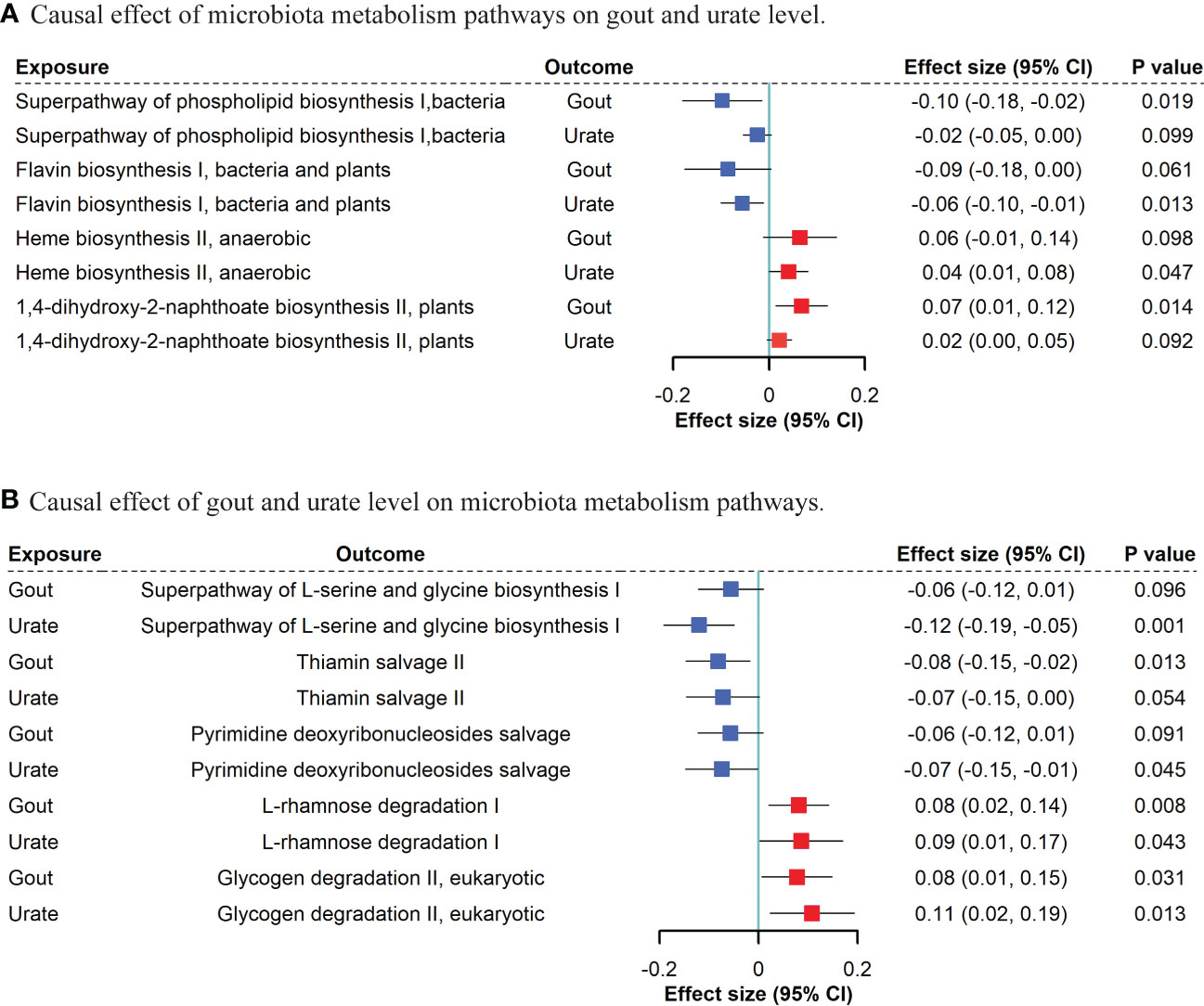
Figure 4 Bidirectional MR suggestive causal association between microbiota metabolism pathways and gout/urate level. (A). Causal effect of microbiota metabolism pathways on gout and urate level. (B). Causal effect of gout and urate level on microbiota metabolism pathways. We included “suggestive” significant pathways in Figure 4 (P <0.05 in gout or urate level and P <0.1 with the same direction in the other phenotype).
图 4 微生物群代谢途径与痛风/尿酸水平之间的双向 MR 提示性因果关系。(A).微生物群代谢途径对痛风和尿酸水平的因果效应。(B).痛风和尿酸水平对微生物群代谢途径的因果效应。我们在图 4 中列出了 "提示性 "的重要途径(痛风或尿酸水平的 P <0.05,其他表型的同方向 P <0.1)。
For gout and urate level on microbiota, we found that both gout presence and urate level had a causal effect on bacterial L-rhamnose degradation (gout: β: 0.08, 95% CI: [0.02, 0.14], P = 0.008; urate level: β: 0.09, 95% CI: [0.01, 0.17], P = 0.043) and glycogen degradation (gout: β: 0.08, 95% CI: [0.01, 0.15], P = 0.031; urate level: β: 0.11, 95% CI: [0.02, 0.19], P = 0.013). Other five bacterial metabolism pathways affected by gout and nine pathways affected by urate level can be found in Tables S14, S15.
在痛风和尿酸水平对微生物群的影响方面,我们发现痛风的存在和尿酸水平对细菌的 L-鼠李糖降解有因果关系(痛风:β:0.08,95% CI:[0.02,0.14],P = 0.008;尿酸水平:β:0.09,95% CI:[0.01,0.17],P = 0.043)和糖原降解(痛风:β:0.08,95% CI:[0.01,0.15],P = 0.031;尿酸水平:β:0.11,95% CI:[0.02,0.19],P = 0.013)。受痛风影响的其他 5 个细菌代谢途径和受尿酸水平影响的 9 个途径见表 S14 和 S15。
Among all 1654 analyses, 80 non-significant results with Egger intercept P <0.05 were excluded. Little pleiotropy remained in the remaining significant results (Table S16). Among all 3318 analyses, 196 non-significant IVW results with Cochrane’s Q test P <0.05 were excluded. Little heterogeneity remained in the significant results (Table S17).
在所有 1654 项分析中,剔除了 80 项 Egger 截距 P <0.05 的非显著结果。剩余的显著结果中几乎不存在多重效应(表 S16)。在所有 3318 项分析中,排除了 196 项 Cochrane's Q 检验 P <0.05 的非显著 IVW 结果。有意义的结果几乎没有异质性(表 S17)。
3.3 Mediation analysis of microbiota, DHA, and gout/urate level
3.3 微生物群、DHA 和痛风/尿酸水平的中介分析
Firstly, DHA had a significant causal effect on both gout (β: -0.09, 95% CI: [-0.17, -0.01], P =0.021) and urate level (β: -0.07, 95% CI: [-0.11, -0.03], P <0.001). Secondly, given the protected effect of DHA, among 19 taxa causally associated with gout or urate level, Bifidobacteriales order and Bifidobacteriaceae family (both β: 0.06, 95% CI: [0.01, 0.13], P =0.044) were positively associated with DHA level and negatively associated with urate level (β: -0.06, 95% CI: [-0.11, -0.01], P =0.020) (Table S18). In the mediation analysis, the indirect effect of Bifidobacteriales order on urate level via DHA was (β: -0.004, 95% CI: [-0.003, -0.01]) and the proportion of DHA mediation was 7.6% (P =0.016). Consistent with DHA, PUFAs level also had a causal effect on both gout (β: -0.40, 95% CI: [-0.62, -0.18], P <0.001) and urate level (β: -0.21, 95% CI: [-0.29, -0.12], P <0.001), while the Bifidobacteriales order and Bifidobacteriaceae family had a significant causal effect on serum PUFAs level (both β: 0.04, 95% CI: [0.01, 0.08], P =0.010) (Table S19). However, the indirect effect of the Bifidobacteriales order on urate level via PUFAs was not statistically significant (β: -0.0097, 95% CI: [-0.020, 0.034], P =0.667).
首先,DHA 对痛风(β:-0.09,95% CI:[-0.17,-0.01],P =0.021)和尿酸水平(β:-0.07,95% CI:[-0.11,-0.03],P <0.001)均有显著的因果关系。其次,鉴于 DHA 的保护效应,在 19 个与痛风或尿酸水平有因果关系的类群中,双歧杆菌目和双歧杆菌科(β:均为 0.06,95% CI:[0.01,0.13],P =0.044)与 DHA 水平呈正相关,而与尿酸水平呈负相关(β:-0.06,95% CI:[-0.11,-0.01],P =0.020)(表 S18)。在中介分析中,双歧杆菌顺序通过 DHA 对尿酸水平的间接影响为(β:-0.004,95% CI:[-0.003,-0.01]),DHA 的中介比例为 7.6%(P =0.016)。与 DHA 一致,PUFAs 水平对痛风(β:-0.40,95% CI:[-0.62,-0.18],P <0.001)和尿酸水平(β:-0.21,95% CI:[-0.29,-0.12],P <0.001),而双歧杆菌目和双歧杆菌科对血清 PUFAs 水平有显著的因果效应(β:均为 0.04,95% CI:[0.01,0.08],P =0.010)(表 S19)。然而,双歧杆菌顺序通过 PUFAs 对尿酸水平的间接影响在统计学上并不显著(β:-0.0097,95% CI:[-0.020,0.034],P =0.667)。
We then estimated the causal effect of the Bifidobacteriales order and Bifidobacteriaceae family on urate level under a stricter significance threshold of IVs (P <1×10-8). The Wald ratio showed the only remaining rs182549 (P =5.9×10-20) had a significant causal effect on DHA level (β: 0.22, 95% CI: [0.15, 0.30], P <0.001). We then accessed the colocalization evidence to the 5000 bp region encompassing the SNP rs182549 at MCM6 locus using the summary statistics from Bifidobacteriales order and Bifidobacteriaceae family, DHA, and urate level. The colocalization posterior probability (H4) of COLOC is high with 0.999 in both DHA and urate, which indicated the Bifidobacteriales order and Bifidobacteriaceae family shared a specific common variant rs182549 with both DHA and urate. We then searched the PhenoScanner database for rs182549 and mapped this variant in the MCM6 gene combined with LCT in the pQTL analysis.
然后,我们在更严格的IV显著性阈值(P <1×10 -8 )下估计了双歧杆菌目和双歧杆菌科对尿酸水平的因果效应。Wald比值显示,仅剩下rs182549(P =5.9×10 -20 )对DHA水平有显著的因果效应(β:0.22,95% CI:[0.15,0.30],P <0.001)。然后,我们利用双歧杆菌目和双歧杆菌科、DHA 和尿酸水平的汇总统计,对 MCM6 基因座上包含 SNP rs182549 的 5000 bp 区域进行了共定位证据分析。COLOC的共定位后验概率(H4)在DHA和尿酸盐中都高达0.999,这表明双歧杆菌目和双歧杆菌科在DHA和尿酸盐中都有一个特定的共同变异体rs182549。随后,我们在 PhenoScanner 数据库中搜索了 rs182549,并在 pQTL 分析中将该变异映射到了 MCM6 基因与 LCT 的结合处。
4 Discussion 4 讨论
In the present study, we found that 20 genetically predicted taxa significantly affected urate metabolism, and 29 taxa were affected by urate metabolism, followed by supportive genetic correlation from LDSC. Two taxa had a common causal effect on both gout and urate, whereas the Victivallaceae family was replicable in the independent GUGC cohort. Six taxa were commonly affected by both gout and urate, whereas the Ruminococcus gnavus group genus was replicable in the GUGC. DHA may mediate the protective effect of Bifidobacteriales order and Bifidobacteriaceae family on the host urate level. Bifidobacteriales order and Bifidobacteriaceae family shared a common causal variant rs182549 associated with MCM6/LCT with both DHA and urate level. To our knowledge, this is the first study to comprehensively examine the genetic association between gut microbiota and urate metabolism. Our findings implicated the critical role of gut microorganisms in host-microbiota crosstalk of urate metabolism disorders, underlying the importance of modulating host-microbe balance in the prevention and treatment of hyperuricemia diseases.
在本研究中,我们发现 20 个遗传预测类群对尿酸盐代谢有显著影响,29 个类群受尿酸盐代谢影响,其次是来自 LDSC 的支持性遗传相关性。有两个类群对痛风和尿酸盐均有共同的因果影响,而维克瓦里科在独立的 GUGC 队列中具有可复制性。有六个类群同时受到痛风和尿酸盐的共同影响,而 Ruminococcus gnavus 群属可在 GUGC 中复制。DHA可能介导了双歧杆菌目和双歧杆菌科对宿主尿酸水平的保护作用。双歧杆菌目和双歧杆菌科有一个共同的因果变异体 rs182549,它与 DHA 和尿酸水平有关的 MCM6/LCT 相关。据我们所知,这是第一项全面研究肠道微生物群与尿酸盐代谢之间遗传关联的研究。我们的研究结果表明,肠道微生物在尿酸盐代谢紊乱的宿主-微生物群串联中发挥着关键作用,这也揭示了调节宿主-微生物平衡在预防和治疗高尿酸血症疾病中的重要性。
Gut microbiota plays an essential role in the production, catabolism, metabolism, and excretion of host uric acid. It could either convert purines to uric acid by secreting active enzymes or accelerate uric acid degradation by synthesizing urate-metabolizing enzymes (37). However, most studies focusing on the interaction of gut microbiota and uric acid metabolism were cross-sectional studies, which could hardly determine the chronological order of the change in uric acid level and microbiota abundance (7–10). For example, elevated serum urate level could be related to the change in abundance of both purine-decomposition and purine-synthesis bacteria (5). Whether this change in abundance is pathogenic or compensatory for hyperuricemia remains unclear. The present study used bidirectional MR and MR Steiger direction tests to ensure the right causal direction between microbiota and urate metabolism (38). We found that the Victivallaceae family and Lachnospiraceae ND3007 group genus had a causal effect on both gout and urate level. The former taxon has not been well investigated, while the latter taxon belonged to an important disease-inducing family, the Lachnospiraceae family (39). Our MR results indicated five genera in this family had causal effects on gout or urate metabolism. However, the negative results of other taxa in the Lachnospiraceae family were not insignificant. Due to the controversial role of different inferior genera, function-dependent cluster analysis or taxon-to-taxon ratio on urate metabolism is warranted for further investigation (39).
肠道微生物群在宿主尿酸的产生、分解、代谢和排泄过程中发挥着重要作用。它可以通过分泌活性酶将嘌呤转化为尿酸,也可以通过合成尿酸代谢酶加速尿酸降解(37)。然而,大多数关注肠道微生物群与尿酸代谢相互作用的研究都是横断面研究,很难确定尿酸水平和微生物群丰度变化的时间顺序(7-10)。例如,血清尿酸水平升高可能与嘌呤分解菌和嘌呤合成菌的丰度变化有关(5)。这种丰度变化是致病性的还是高尿酸血症的代偿性的仍不清楚。本研究采用了双向 MR 和 MR Steiger 方向检验,以确保微生物群与尿酸盐代谢之间的因果关系方向正确(38)。我们发现,Victivallaceae 科和 Lachnospiraceae ND3007 群属对痛风和尿酸水平均有因果关系。前一个类群尚未得到很好的研究,而后一个类群属于一个重要的致病科--Lachnospiraceae 科(39)。我们的 MR 结果表明,该科中有五个属对痛风或尿酸盐代谢有因果影响。不过,Lachnospiraceae 科中其他类群的负面结果也不小。由于不同下位属的作用存在争议,因此有必要对尿酸盐代谢进行功能依赖性聚类分析或类群-类群比进行进一步研究(39)。
In turn, gout and hyperuricemia could also trigger variations in gut microbiota abundance and metabolism. Consistent with observatory studies, the abundance of the Coriobacteriaceae family, Prevotellaceae family, Lachnoclostridium genus, and Bacteroides genus changed in patients with gout during treatment (9, 40–42). Therefore, similar to biomarkers of specific diseases, microbial dysbiosis and metabolic disorders serve as a profound reference for future studies in uric metabolism. Patients’ fecal microbiome could be considered a pre-diagnostic target of gout and hyperuricemia (43).
反过来,痛风和高尿酸血症也可能引发肠道微生物群丰度和代谢的变化。与观察性研究一致,痛风患者在治疗过程中,冠状杆菌科(Coriobacteriaceae)、前鞭毛菌科(Prevotellaceae)、Lachnoclostridium属(Lachnoclostridium)和Bacteroides属(Bacteroides)的丰度发生了变化(9,40- 42)。因此,与特定疾病的生物标志物类似,微生物菌群失调和代谢紊乱也是今后研究尿酸代谢的重要参考依据。患者的粪便微生物组可被视为痛风和高尿酸血症的预诊断目标(43)。
Our results highlighted the different profiles of significant taxa in gout and urate level. Hyperuricemia and gout share common characteristics but also have differences. While a large proportion of individuals with hyperuricemia have never had a gout flare, some patients with gout can have a normuricemia status (44, 45). Hyperuricemia is generally considered to be the pathophysiologic basis of gout flares, and uric acid has dual effects in vivo with antioxidant properties as well as being an inflammatory promoter, which places it in a delicate position in balancing metabolisms (46). On the other hand, gout is a multifactorial metabolic disease, and its pathogenesis should not rely solely on hyperuricemia or monosodium urate crystals (46). Thus, the spectrum of significant taxa, combined with the mediation effect of DHA of hyperuricemia was quite different from that of gout; this might explain the difference between gout and urate metabolism in the MR analysis.
我们的研究结果突显了痛风和尿酸水平中重要类群的不同特征。高尿酸血症和痛风具有共同的特征,但也存在差异。大部分高尿酸血症患者从未出现过痛风发作,而一些痛风患者的尿酸血症状态可能正常(44,45)。高尿酸血症通常被认为是痛风发作的病理生理基础,尿酸在体内具有抗氧化和促进炎症的双重作用,这使其在平衡新陈代谢中处于微妙的地位(46)。另一方面,痛风是一种多因素代谢性疾病,其发病机制不应仅依赖于高尿酸血症或单钠尿酸盐结晶(46)。因此,高尿酸血症的重要类群谱以及 DHA 的中介效应与痛风的类群谱截然不同;这可能解释了 MR 分析中痛风与尿酸盐代谢之间的差异。
Bifidobacteria is a well-known probiotic to treat hyperuricemia, which is consistent with our MR (47). Studies indicated that Bifidobacteria supplement could elevate DHA levels in animal experiments and DHA supplement could improve hyperuricemia in humans (12, 48). We found that both the Bifidobacteriales order and Bifidobacteriaceae family had a protective effect on urate metabolism partially through DHA level, whereas rs182549 in MCM6 was the most predominant variant. MCM6 could be activated by both DHA supplements in the human body and hyperuricemia status in mice (49, 50). The complex MCM6/LCT variation also participated in several diseases’ progress such as obesity, lactose intolerance, and irritable bowel syndrome (51, 52). This suggested that rs182549, which is related to Bifidobacteria, might play a critical role in the interplay of gut microbiota, unsaturated fatty acid, and urate metabolism. Furthermore, MCM6/LCT might be a potential therapeutic target for treating hyperuricemia.
双歧杆菌是众所周知的治疗高尿酸血症的益生菌,这与我们的 MR ( 47) 一致。研究表明,在动物实验中补充双歧杆菌可以提高 DHA 水平,而补充 DHA 可以改善人类的高尿酸血症(12,48)。我们发现,双歧杆菌目和双歧杆菌科细菌部分通过 DHA 水平对尿酸盐代谢具有保护作用,而 MCM6 中的 rs182549 是最主要的变异。人体补充 DHA 和小鼠高尿酸血症状态都会激活 MCM6(49,50)。复杂的 MCM6/LCT 变异也参与了多种疾病的进展,如肥胖、乳糖不耐症和肠易激综合征 ( 51, 52)。这表明,与双歧杆菌相关的 rs182549 可能在肠道微生物群、不饱和脂肪酸和尿酸盐代谢的相互作用中发挥关键作用。此外,MCM6/LCT 可能是治疗高尿酸血症的潜在治疗靶点。
Although gut microbiota was previously thought to be influenced by host health status, the GWAS significant variants representing the microbiota phenotype were relatively not largely confounded (19). Also, we assessed the genetic effect of microbiota in both gout and urate level. These two statistics were highly correlated but were derived from two independent populations. This not only avoided sample overlap but also replicated MR results in a related phenotype.
虽然肠道微生物群以前被认为会受到宿主健康状况的影响,但代表微生物群表型的 GWAS 重要变异相对来说在很大程度上没有被混淆(19)。此外,我们还评估了微生物群对痛风和尿酸水平的遗传影响。这两项统计高度相关,但来自两个独立的人群。这不仅避免了样本重叠,还复制了 MR 在相关表型中的结果。
This study has several limitations. Firstly, a relatively non-significant heritability of the gut microbiota of the MiBioGen and DMP GWAS might impair the detective power of MR. However, owing to the sufficient sample size of publicly available data from the largest GWAS such as MiBioGen, DMP, and GBMI, the weak instrument bias could be somewhat complemented. Thus, we had adequate power to detect significant lifelong causality. Secondly, due to the difference between gout and urate, it is predictable that some bacteria related to one phenotype could not be replicable in the other phenotype. Therefore, some significant taxa in gout might not be associated with the urate level but might be associated more with systematic inflammation and intestinal transportation (53, 54). This could partly explain the different significant taxa in the two phenotypes.
这项研究有几个局限性。首先,MiBioGen 和 DMP GWAS 的肠道微生物群遗传率相对不显著,这可能会影响 MR 的检测能力。然而,由于来自 MiBioGen、DMP 和 GBMI 等最大 GWAS 的公开数据具有足够的样本量,可以在一定程度上补充微弱的工具偏倚。因此,我们有足够的能力检测出显著的终身因果关系。其次,由于痛风和尿酸盐之间的差异,可以预测一些与一种表型相关的细菌无法在另一种表型中复制。因此,痛风中的一些重要类群可能与尿酸水平无关,而更多地与系统性炎症和肠道运输有关(53,54)。这可以部分解释两种表型中不同的重要类群。
In conclusion, this is the first study comprehensively assessing the association between gut microbiota and urate metabolism based on genetic methods. Our findings underlined the critical role of gut microorganisms in host hyperuricemia pathogenesis and progress. Taking advantage of host-microbiota crosstalk in urate metabolism could not only indicate directions of clinical prediction and the monitoring of gout but also draw a future blueprint for a cutting-edge therapeutic method based on fecal bacteria transplantation.
总之,这是第一项基于遗传学方法全面评估肠道微生物群与尿酸盐代谢之间关系的研究。我们的发现强调了肠道微生物在宿主高尿酸血症发病机制和进展中的关键作用。利用宿主-微生物群在尿酸盐代谢中的串联作用,不仅能为痛风的临床预测和监测指明方向,还能为基于粪菌移植的前沿治疗方法描绘未来蓝图。
Data availability statement
数据可用性声明
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
文章/补充材料中包含了该研究的原创性贡献。如需进一步咨询,请联系通讯作者。
Author contributions 作者供稿
MX, TH, YB and GN conceived and designed the study. TH, QW, HD and YH conducted the analysis and finished writing the paper. XZ, JZ, TW, ML, HL, SW, ZZ, YG and YX offered guidance and methods for the analysis and data selection. YC, JL, WW, GN and YB reviewed the article and offered clinical advice. MX, YB and GN took responsibility for the contents of the article. All authors contributed to the article and approved the submitted version.
MX、TH、YB 和 GN 构思并设计了本研究。TH、QW、HD 和 YH 进行了分析并完成了论文的撰写。XZ、JZ、TW、ML、HL、SW、ZZ、YG 和 YX 为分析和数据选择提供了指导和方法。YC、JL、WW、GN和YB审阅了文章并提供了临床建议。MX、YB和GN对文章内容负责。所有作者都对文章做出了贡献,并批准了提交的版本。
Funding 资金筹措
This work was funded by the National Natural Science Foundation of China (81941017, 82270859, 81930021, 81970728, 91857205, and 82088102), the Shanghai Municipal Education Commission–Gaofeng Clinical Medicine Grant Support (20152508 Round 2), the Shanghai Shenkang Hospital Development Center (SHDC12019101, SHDC2020CR1001A, and SHDC2020CR3069B), the Shanghai Jiao Tong University School of Medicine (DLY201801), and the Ruijin Hospital (2018CR002). MX, ML, TW, YX, JL, YB, WW, and GN are members of innovative research teams of high-level local universities in Shanghai. The study sponsors were not involved in the design of the study; the collection, analysis, and interpretation of data; writing the report; and they did not impose any restrictions regarding the publication of the report.
本研究得到了国家自然科学基金(81941017、82270859、81930021、81970728、91857205和82088102)、上海市教委-高锋临床医学资助项目(20152508第二轮)、上海申康医院发展中心(SHDC12019101、SHDC2020CR1001A和SHDC2020CR3069B)、上海交通大学医学院(DLY201801)和瑞金医院(2018CR002)的资助。MX、ML、TW、YX、JL、YB、WW 和 GN 为上海本地高水平大学创新研究团队成员。研究赞助方未参与研究的设计、数据的收集、分析和解释以及报告的撰写,也未对报告的发表施加任何限制。
Acknowledgments 致谢
In this study, we used GWAS summary data from the MiBioGen, Dutch Microbiome Project, GBMI consortium, GUGC consortium, and the IEU OpenGWAS project. We thank all the investigators who provided these data to support this study and the individual patients who provided the sample that made the data available; without them, the study would not have been possible. We also express our gratitude to Miss. Mingqing Yuan from Zhejiang University for making the figures.
在本研究中,我们使用了来自 MiBioGen、荷兰微生物组项目、GBMI 联盟、GUGC 联盟和 IEU OpenGWAS 项目的 GWAS 摘要数据。我们感谢所有提供这些数据以支持本研究的研究者,以及提供样本以获得数据的患者个人;没有他们,本研究就不可能进行。我们还要感谢浙江大学的袁明清老师。浙江大学的 Mingqing Yuan 小姐制作了图表。
Conflict of interest 利益冲突
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
作者声明,本研究在进行过程中不存在任何可能被视为潜在利益冲突的商业或经济关系。
Publisher’s note 出版商说明
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
本文中表述的所有主张仅代表作者本人,并不一定代表其附属机构的主张,也不代表出版商、编辑和审稿人的主张。本文可能评估的任何产品,或其制造商可能提出的任何主张,均未得到出版商的保证或认可。
Supplementary material 补充材料
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1148591/full#supplementary-material
本文的补充材料可在线查阅: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1148591/full#supplementary-material
References 参考资料
1. Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout. Lancet (2021) 397(10287):1843–55. doi: 10.1016/S0140-6736(21)00569-9
1.Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout.柳叶刀(2021)397(10287):1843-55。DOI:10.1016/S0140-6736(21)00569-9
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
2. Cipolletta E, Tata LJ, Nakafero G, Avery AJ, Mamas MA, Abhishek A. Association between gout flare and subsequent cardiovascular events among patients with gout. Jama. (2022) 328(5):440–50. doi: 10.1001/jama.2022.11390
2.Cipolletta E、Tata LJ、Nakafero G、Avery AJ、Mamas MA、Abhishek A. 痛风患者痛风发作与后续心血管事件之间的关系。牙买加。(doi: 10.1001/jama.2022.11390.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
3. Jakše B, Jakše B, Pajek M, Pajek J. Uric acid and plant-based nutrition. Nutrients. (2019) 11(8):1736. doi: 10.3390/nu11081736
3.Jakše B、Jakše B、Pajek M、Pajek J.《尿酸与植物营养》。Nutrients.(2019) 11(8):1736. doi: 10.3390/nu11081736
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
4. Tong S, Zhang P, Cheng Q, Chen M, Chen X, Wang Z, et al. The role of gut microbiota in gout: Is gut microbiota a potential target for gout treatment. Front Cell Infect Microbiol (2022) 12:1051682. doi: 10.3389/fcimb.2022.1051682
4.Tong S, Zhang P, Cheng Q, Chen M, Chen X, Wang Z, et al:肠道微生物群是痛风治疗的潜在靶点吗?Doi: 10.3389/fcimb.2022.1051682.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
5. Yu Y, Liu Q, Li H, Wen C, He Z. Alterations of the gut microbiome associated with the treatment of hyperuricaemia in Male rats. Front Microbiol (2018) 9:2233. doi: 10.3389/fmicb.2018.02233
5.Yu Y, Liu Q, Li H, Wen C, He Z. 与雄性大鼠高尿酸血症治疗相关的肠道微生物组变化。Front Microbiol (2018) 9:2233. doi: 10.3389/fmicb.2018.02233
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
6. Gu Y, Wang X, Li J, Zhang Y, Zhong H, Liu R, et al. Analyses of gut microbiota and plasma bile acids enable stratification of patients for antidiabetic treatment. Nat Commun (2017) 8(1):1785. doi: 10.1038/s41467-017-01682-2
6.Gu Y, Wang X, Li J, Zhang Y, Zhong H, Liu R, et al. 分析肠道微生物群和血浆胆汁酸可对患者进行抗糖尿病治疗分层。Nat Commun (2017) 8(1):1785. doi: 10.1038/s41467-017-01682-2
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
7. Méndez-Salazar EO, Vázquez-Mellado J, Casimiro-Soriguer CS, Dopazo J, Çubuk C, Zamudio-Cuevas Y, et al. Taxonomic variations in the gut microbiome of gout patients with and without tophi might have a functional impact on urate metabolism. Mol Med (2021) 27(1):50. doi: 10.1186/s10020-021-00311-5
7.Méndez-Salazar EO、Vázquez-Mellado J、Casimiro-Soriguer CS、Dopazo J、Çubuk C、Zamudio-Cuevas Y 等:有和无趾骨痛风患者肠道微生物组的分类变异可能对尿酸盐代谢有功能性影响。DOI: 10.1186/s10020-021-00311-5
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
8. Kim HW, Yoon EJ, Jeong SH, Park MC. Distinct gut microbiota in patients with asymptomatic hyperuricemia: A potential protector against gout development. Yonsei Med J (2022) 63(3):241–51. doi: 10.3349/ymj.2022.63.3.241
8.Kim HW, Yoon EJ, Jeong SH, Park MC.无症状高尿酸血症患者体内独特的肠道微生物群:防止痛风发生的潜在保护器。Doi: 10.3349/ymj.2022.63.3.241.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
9. Park HK, Lee SJ. Treatment of gouty arthritis is associated with restoring the gut microbiota and promoting the production of short-chain fatty acids. Arthritis Res Ther (2022) 24(1):51. doi: 10.1186/s13075-022-02742-9
9.Park HK, Lee SJ.痛风性关节炎的治疗与恢复肠道微生物群和促进短链脂肪酸的产生有关。Arthritis Res Ther (2022) 24(1):51. doi: 10.1186/s13075-022-02742-9
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
10. Guo Z, Zhang J, Wang Z, Ang KY, Huang S, Hou Q, et al. Intestinal microbiota distinguish gout patients from healthy humans. Sci Rep (2016) 6:20602. doi: 10.1038/srep20602
10.Guo Z, Zhang J, Wang Z, Ang KY, Huang S, Hou Q, et al.科学报告(2016)6:20602.doi: 10.1038/srep20602
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
11. Abdollahi-Roodsaz S, Abramson SB, Scher JU. The metabolic role of the gut microbiota in health and rheumatic disease: mechanisms and interventions. Nat Rev Rheumatol (2016) 12(8):446–55. doi: 10.1038/nrrheum.2016.68
11.Abdollahi-Roodsaz S, Abramson SB, Scher JU.肠道微生物群在健康和风湿病中的代谢作用:机制与干预。Nat Rev Rheumatol (2016) 12(8):446-55. doi: 10.1038/nrrheum.2016.68
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
12. Saito H, Toyoda Y, Takada T, Hirata H, Ota-Kontani A, Miyata H, et al. Omega-3 polyunsaturated fatty acids inhibit the function of human URAT1, a renal urate re-absorber. Nutrients (2020) 12(6):1601. doi: 10.3390/nu12061601
12.Saito H, Toyoda Y, Takada T, Hirata H, Ota-Kontani A, Miyata H, et al. Omega-3 多不饱和脂肪酸抑制肾尿酸重吸收器人 URAT1 的功能。营养素(2020)12(6):1601。
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
13. Zhang M, Zhang Y, Terkeltaub R, Chen C, Neogi T. Effect of dietary and supplemental omega-3 polyunsaturated fatty acids on risk of recurrent gout flares. Arthritis Rheumatol (2019) 71(9):1580–6. doi: 10.1002/art.40896
13.Zhang M、Zhang Y、Terkeltaub R、Chen C、Neogi T.膳食和补充ω-3多不饱和脂肪酸对痛风复发风险的影响。Arthritis Rheumatol (2019) 71(9):1580-6. doi: 10.1002/art.40896
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
14. Abhishek A, Valdes AM, Doherty M. Low omega-3 fatty acid levels associate with frequent gout attacks: a case control study. Ann Rheum Dis (2016) 75(4):784–5. doi: 10.1136/annrheumdis-2015-208767
14.Abhishek A、Valdes AM、Doherty M.低ω-3脂肪酸水平与痛风频繁发作有关:一项病例对照研究。Doi: 10.1136/annrheumdis-2015-208767.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
15. Stamp LK, Grainger R, Frampton C, Drake J, Hill CL. Effect of omega-three supplementation on serum urate and gout flares in people with gout; a pilot randomized trial. BMC Rheumatol (2022) 6(1):31. doi: 10.1186/s41927-022-00263-1
15.Stamp LK, Grainger R, Frampton C, Drake J, Hill CL.补充欧米伽三对痛风患者血清尿酸盐和痛风发作的影响;一项试点随机试验。DOI: 10.1186/s41927-022-00263-1
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
16. Miyamoto J, Igarashi M, Watanabe K, Karaki SI, Mukouyama H, Kishino S, et al. Gut microbiota confers host resistance to obesity by metabolizing dietary polyunsaturated fatty acids. Nat Commun (2019) 10(1):4007. doi: 10.1038/s41467-019-11978-0
16.Miyamoto J, Igarashi M, Watanabe K, Karaki SI, Mukouyama H, Kishino S, et al. Gut microbiota confers host resistance to obesity by metabolizing dietary polyunsaturated fatty acids.Nat Commun (2019) 10(1):4007. doi: 10.1038/s41467-019-11978-0
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
17. Skrivankova VW, Richmond RC, Woolf BAR, Davies NM, Swanson SA, VanderWeele TJ, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomisation (STROBE-MR): Explanation and elaboration. BMJ (2021) 375:n2233. doi: 10.1136/bmj.n2233
17.Skrivankova VW, Richmond RC, Woolf BAR, Davies NM, Swanson SA, VanderWeele TJ, et al:解释与阐述。BMJ (2021) 375:n2233.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
18. Kurilshikov A, Medina-Gomez C, Bacigalupe R, Radjabzadeh D, Wang J, Demirkan A, et al. Large-Scale association analyses identify host factors influencing human gut microbiome composition. Nat Genet (2021) 53(2):156–65. doi: 10.1038/s41588-020-00763-1
18.Kurilshikov A, Medina-Gomez C, Bacigalupe R, Radjabzadeh D, Wang J, Demirkan A, et al. Large-Scale association analyses identify host factors influencing human gut microbiome composition.doi: 10.1038/s41588-020-00763-1
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
19. Lopera-Maya EA, Kurilshikov A, van der Graaf A, Hu S, Andreu-Sánchez S, Chen L, et al. Effect of host genetics on the gut microbiome in 7,738 participants of the Dutch microbiome project. Nat Genet (2022) 54(2):143–51. doi: 10.1038/s41588-021-00992-y
19.Lopera-Maya EA, Kurilshikov A, van der Graaf A, Hu S, Andreu-Sánchez S, Chen L, et al. 宿主遗传对荷兰微生物组项目 7738 名参与者肠道微生物组的影响。doi: 10.1038/s41588-021-00992-y
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
20. Zhou W, Kanai M, Wu KH, Rasheed H, Tsuo K, Hirbo JB, et al. Global biobank meta-analysis initiative: Powering genetic discovery across human disease. Cell Genom (2022) 2(10):100192. doi: 10.1016/j.xgen.2022.100192
20.Zhou W, Kanai M, Wu KH, Rasheed H, Tsuo K, Hirbo JB, et al:为人类疾病的基因发现提供动力。Doi: 10.1016/j.xgen.2022.100192.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
21. Tin A, Marten J, Halperin Kuhns VL, Li Y, Wuttke M, Kirsten H, et al. Target genes, variants, tissues and transcriptional pathways influencing human serum urate levels. Nat Genet (2019) 51(10):1459–74. doi: 10.1038/s41588-019-0504-x
21.Tin A, Marten J, Halperin Kuhns VL, Li Y, Wuttke M, Kirsten H, et al. Target genes, variants, tissues and transcriptional pathways influencing human serum urate levels.Nat Genet (2019) 51(10):1459-74. doi: 10.1038/s41588-019-0504-x
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
22. Köttgen A, Albrecht E, Teumer A, Vitart V, Krumsiek J, Hundertmark C, et al. Genome-wide association analyses identify 18 new loci associated with serum urate concentrations. Nat Genet (2013) 45(2):145–54. doi: 10.1038/ng.2500
22.Köttgen A, Albrecht E, Teumer A, Vitart V, Krumsiek J, Hundertmark C, et al. Genome-wide association analyses identify 18 new loci associated with serum urate concentrations.Nat Genet (2013) 45(2):145-54. Doi: 10.1038/ng.2500
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
23. Richardson TG, Leyden GM, Wang Q, Bell JA, Elsworth B, Davey Smith G, et al. Characterising metabolomic signatures of lipid-modifying therapies through drug target mendelian randomisation. PloS Biol (2022) 20(2):e3001547. doi: 10.1371/journal.pbio.3001547
23.Richardson TG, Leyden GM, Wang Q, Bell JA, Elsworth B, Davey Smith G, et al.PloS Biol (2022) 20(2):e3001547. doi: 10.1371/journal.pbio.3001547
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
24. Hemani G, Zheng J, Elsworth B, Wade KH, Haberland V, Baird D, et al. The MR-base platform supports systematic causal inference across the human phenome. Elife (2018) 7:e34408. doi: 10.7554/eLife.34408
24.Hemani G, Zheng J, Elsworth B, Wade KH, Haberland V, Baird D, et al. MR-base platform supports systematic causal inference across the human phenome.Elife (2018) 7:e34408. doi: 10.7554/eLife.34408
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
25. Hou T, Li M, Lin H, Zhao Z, Lu J, Wang T, et al. The causal effect of systolic blood pressure lowering on vascular outcomes in diabetes: a mendelian randomization study. J Clin Endocrinol Metab (2022) 107(9):2616–25. doi: 10.1210/clinem/dgac354
25.Hou T, Li M, Lin H, Zhao Z, Lu J, Wang T, et al. 降低收缩压对糖尿病血管预后的因果效应:泯灭随机研究。J Clin Endocrinol Metab (2022) 107(9):2616-25. doi: 10.1210/clinem/dgac354
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
26. Sudmant PH, Rausch T, Gardner EJ, Handsaker RE, Abyzov A, Huddleston J, et al. An integrated map of structural variation in 2,504 human genomes. Nature (2015) 526(7571):75–81. doi: 10.1038/nature15394
26.Sudmant PH、Rausch T、Gardner EJ、Handsaker RE、Abyzov A、Huddleston J 等:2504 个人类基因组结构变异的综合图谱。doi: 10.1038/nature15394.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
27. Burgess S, Small DS, Thompson SG. A review of instrumental variable estimators for mendelian randomization. Stat Methods Med Res (2017) 26(5):2333–55. doi: 10.1177/0962280215597579
27.Burgess S, Small DS, Thompson SG.孟德尔随机化工具变量估计器综述。Stat Methods Med Res (2017) 26(5):2333-55. doi: 10.1177/0962280215597579
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
28. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. (2016) 40(4):304–14. doi: 10.1002/gepi.21965
28.Bowden J, Davey Smith G, Haycock PC, Burgess S. 使用加权中位数估计器对某些无效工具的泯灭随机化进行一致估计。Genet Epidemiol.(doi: 10.1002/gepi.21965.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
29. Burgess S, Thompson SG. Interpreting findings from mendelian randomization using the MR-egger method. Eur J Epidemiol. (2017) 32(5):377–89. doi: 10.1007/s10654-017-0255-x
29.Burgess S, Thompson SG.使用 MR-egger 方法解读 "泯灭随机 "的研究结果。Eur J Epidemiol.(2017) 32(5):377-89. doi: 10.1007/s10654-017-0255-x
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
30. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from mendelian randomization between complex traits and diseases. Nat Genet (2018) 50(5):693–8. doi: 10.1038/s41588-018-0099-7
30.Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from mendelian randomization between complex traits and diseases.Doi: 10.1038/s41588-018-0099-7.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
31. Burgess S, Foley CN, Allara E, Staley JR, Howson JMM. A robust and efficient method for mendelian randomization with hundreds of genetic variants. Nat Commun (2020) 11(1):376. doi: 10.1038/s41467-019-14156-4
31.Burgess S, Foley CN, Allara E, Staley JR, Howson JMM.具有数百个遗传变异的稳健高效的泯灭随机化方法。doi: 10.1038/s41467-019-14156-4
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
32. Shen B, Li Y, Sheng CS, Liu L, Hou T, Xia N, et al. Association between age at diabetes onset or diabetes duration and subsequent risk of pancreatic cancer: Results from a longitudinal cohort and mendelian randomization study. Lancet Reg Health West Pac. (2023) 30:100596. doi: 10.1016/j.lanwpc.2022.100596
32.Shen B, Li Y, Sheng CS, Liu L, Hou T, Xia N, et al:一项纵向队列和孟德尔随机研究的结果。doi: 10.1016/j.lanwpc.2022.100596.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
33. Carter AR, Gill D, Davies NM, Taylor AE, Tillmann T, Vaucher J, et al. Understanding the consequences of education inequality on cardiovascular disease: mendelian randomisation study. BMJ (2019) 365:l1855. doi: 10.1136/bmj.l1855
33.Carter AR, Gill D, Davies NM, Taylor AE, Tillmann T, Vaucher J, et al. Understanding the consequences of education inequality on cardiovascular disease: mendelian randomisation study.BMJ (2019) 365:l1855. doi: 10.1136/bmj.l1855
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
34. Xu M, Zheng J, Hou T, Lin H, Wang T, Wang S, et al. SGLT2 inhibition, choline metabolites, and cardiometabolic diseases: A mediation mendelian randomization study. Diabetes Care (2022) 45(11):2718–28. doi: 10.2337/dc22-0323
34.SGLT2 抑制、胆碱代谢物与心脏代谢疾病:一项调解泯灭随机化研究。Diabetes Care (2022) 45(11):2718-28. doi: 10.2337/dc22-0323
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
35. Bulik-Sullivan B, Finucane HK, Anttila V, Gusev A, Day FR, Loh PR, et al. An atlas of genetic correlations across human diseases and traits. Nat Genet (2015) 47(11):1236–41. doi: 10.1038/ng.3406
35.Bulik-Sullivan B, Finucane HK, Anttila V, Gusev A, Day FR, Loh PR, et al. An atlas of genetic correlations across human diseases and traits.Nat Genet (2015) 47(11):1236-41. doi: 10.1038/ng.3406
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
36. Wallace C. A more accurate method for colocalisation analysis allowing for multiple causal variants. PloS Genet (2021) 17(9):e1009440. doi: 10.1371/journal.pgen.1009440
36.Wallace C. 允许多因果变异的更精确的共定位分析方法。PloS Genet (2021) 17(9):e1009440. doi: 10.1371/journal.pgen.1009440
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
37. Wang J, Chen Y, Zhong H, Chen F, Regenstein J, Hu X, et al. The gut microbiota as a target to control hyperuricemia pathogenesis: Potential mechanisms and therapeutic strategies. Crit Rev Food Sci Nutr (2022) 62(14):3979–89. doi: 10.1080/10408398.2021.1874287
37.Wang J, Chen Y, Zhong H, Chen F, Regenstein J, Hu X, et al:潜在的机制和治疗策略。Doi: 10.1080/10408398.2021.1874287.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
38. Zheng J, Haberland V, Baird D, Walker V, Haycock PC, Hurle MR, et al. Phenome-wide mendelian randomization mapping the influence of the plasma proteome on complex diseases. Nat Genet (2020) 52(10):1122–31. doi: 10.1038/s41588-020-0682-6
38.Zheng J, Haberland V, Baird D, Walker V, Haycock PC, Hurle MR, et al.Doi: 10.1038/s41588-020-0682-6.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
39. Vacca M, Celano G, Calabrese FM, Portincasa P, Gobbetti M, De Angelis M. The controversial role of human gut lachnospiraceae. Microorganisms (2020) 8(4):573. doi: 10.3390/microorganisms8040573
39.Vacca M, Celano G, Calabrese FM, Portincasa P, Gobbetti M, De Angelis M. The controversial role of human gut lachnospiraceae.doi: 10.3390/microorganisms8040573.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
40. Lv Q, Xu D, Zhang X, Yang X, Zhao P, Cui X, et al. Association of hyperuricemia with immune disorders and intestinal barrier dysfunction. Front Physiol (2020) 11:524236. doi: 10.3389/fphys.2020.524236
40.Lv Q, Xu D, Zhang X, Yang X, Zhao P, Cui X, et al. 高尿酸血症与免疫紊乱和肠屏障功能障碍的关系。Doi: 10.3389/fphys.2020.524236.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
41. Lin X, Shao T, Huang L, Wen X, Wang M, Wen C, et al. Simiao decoction alleviates gouty arthritis by modulating proinflammatory cytokines and the gut ecosystem. Front Pharmacol (2020) 11:955. doi: 10.3389/fphar.2020.00955
41.Lin X, Shao T, Huang L, Wen X, Wang M, Wen C, et al. Simiao decoction alleviates gouty arthritis by modulating proinflammatory cytokines and the gut ecosystem.doi: 10.3389/fphar.2020.00955
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
42. Chu Y, Sun S, Huang Y, Gao Q, Xie X, Wang P, et al. Metagenomic analysis revealed the potential role of gut microbiome in gout. NPJ Biofilms Microbiomes (2021) 7(1):66. doi: 10.1038/s41522-021-00235-2
42.元基因组分析揭示了肠道微生物组在痛风中的潜在作用。NPJ Biofilms Microbiomes (2021) 7(1):66. doi: 10.1038/s41522-021-00235-2
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
43. Li J, Zhao F, Wang Y, Chen J, Tao J, Tian G, et al. Gut microbiota dysbiosis contributes to the development of hypertension. Microbiome (2017) 5(1):14. doi: 10.1186/s40168-016-0222-x
43.Li J, Zhao F, Wang Y, Chen J, Tao J, Tian G, et al. 肠道微生物群失调导致高血压的发生。Microbiome (2017) 5(1):14. doi: 10.1186/s40168-016-0222-x
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
44. Bardin T, Richette P. Definition of hyperuricemia and gouty conditions. Curr Opin Rheumatol (2014) 26(2):186–91. doi: 10.1097/bor.0000000000000028
44.Bardin T, Richette P. 高尿酸血症和痛风的定义。Curr Opin Rheumatol (2014) 26(2):186-91. doi: 10.1097/bor.0000000000000028
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
45. Dalbeth N, House ME, Aati O, Tan P, Franklin C, Horne A, et al. Urate crystal deposition in asymptomatic hyperuricaemia and symptomatic gout: a dual energy CT study. Ann Rheum Dis (2015) 74(5):908–11. doi: 10.1136/annrheumdis-2014-206397
45.Dalbeth N、House ME、Aati O、Tan P、Franklin C、Horne A 等:无症状高尿酸血症和有症状痛风的尿酸盐晶体沉积:双能 CT 研究。Doi: 10.1136/annrheumdis-2014-206397.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
46. Zhang WZ. Why does hyperuricemia not necessarily induce gout? Biomolecules (2021) 11(2):280. doi: 10.3390/biom11020280
46.Zhang WZ.为什么高尿酸血症不一定会诱发痛风?Biomolecules (2021) 11(2):280. doi: 10.3390/biom11020280
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
47. Han J, Wang Z, Lu C, Zhou J, Li Y, Ming T, et al. The gut microbiota mediates the protective effects of anserine supplementation on hyperuricaemia and associated renal inflammation. Food Funct (2021) 12(19):9030–42. doi: 10.1039/d1fo01884a
47.Han J, Wang Z, Lu C, Zhou J, Li Y, Ming T, et al. 肠道微生物群介导补充安赛蜜对高尿酸血症及相关肾脏炎症的保护作用。doi: 10.1039/d1fo01884a
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
48. Bozzi Cionci N, Baffoni L, Gaggìa F, Di Gioia D. Therapeutic microbiology: The role of bifidobacterium breve as food supplement for the Prevention/Treatment of paediatric diseases. Nutrients (2018) 10(11):1723. doi: 10.3390/nu10111723
48.Bozzi Cionci N, Baffoni L, Gaggìa F, Di Gioia D. Therapeutic microbiology:双歧杆菌作为预防/治疗儿科疾病的食品补充剂的作用。Nutrients (2018) 10(11):1723. Doi: 10.3390/nu10111723
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
49. Zhao Z, Zhao Y, Zhang Y, Shi W, Li X, Shyy JY, et al. Gout-induced endothelial impairment: The role of SREBP2 transactivation of YAP. FASEB J (2021) 35(6):e21613. doi: 10.1096/fj.202100337R
49.Zhao Z, Zhao Y, Zhang Y, Shi W, Li X, Shyy JY, et al:SREBP2 对 YAP 的反式激活作用。FASEB J (2021) 35(6):e21613. doi: 10.1096/fj.202100337R
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
50. Myhrstad MC, Ulven SM, Günther CC, Ottestad I, Holden M, Ryeng E, et al. Fish oil supplementation induces expression of genes related to cell cycle, endoplasmic reticulum stress and apoptosis in peripheral blood mononuclear cells: a transcriptomic approach. J Intern Med (2014) 276(5):498–511. doi: 10.1111/joim.12217
50.Myhrstad MC、Ulven SM、Günther CC、Ottestad I、Holden M、Ryeng E 等:鱼油补充会诱导外周血单核细胞中细胞周期、内质网应激和细胞凋亡相关基因的表达:一种转录组学方法。J Intern Med (2014) 276(5):498-511.
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
51. Chiang K-M, Pan W-H. Causal link between milk consumption and obesity? a 10-year longitudinal study and a mendelian randomization study. Food Nutr Res (2021) 65:1–8. doi: 10.29219/fnr.v65.6300
51.Chiang K-M,Pan W-H.牛奶消费与肥胖之间的因果关系?一项为期10年的纵向研究和一项泯灭随机研究。Food Nutr Res (2021) 65:1-8. Doi: 10.29219/fnr.v65.6300
CrossRef Full Text | Google Scholar
全文 | 谷歌学者
52. Almazar AE, Chang JY, Larson JJ, Atkinson EJ, Locke GR, Talley NJ, et al. Comparison of lactase variant MCM6 -13910 C>T testing and self-report of dairy sensitivity in patients with irritable bowel syndrome. J Clin Gastroenterol (2019) 53(6):e227–31. doi: 10.1097/mcg.0000000000001065
52.Almazar AE、Chang JY、Larson JJ、Atkinson EJ、Locke GR、Talley NJ 等:《肠易激综合征患者乳糖酶变异体 MCM6 -13910 C>T 检测与乳制品敏感性自我报告的比较》。J Clin Gastroenterol (2019) 53(6):e227-31. doi: 10.1097/mcg.0000000000001065
PubMed Abstract | CrossRef Full Text | Google Scholar
PubMed 摘要 | CrossRef Full Text | Google Scholar
53. Yin H, Liu N, Chen J. The role of the intestine in the development of hyperuricemia. Front Immunol (2022) 13:845684. doi: 10.3389/fimmu.2022.845684
53.Yin H, Liu N, Chen J. 肠道在高尿酸血症发病中的作用。Doi: 10.3389/fimmu.2022.845684.
Keywords: gout, uric acid, docosahexaenoic acids, mendelian randomization, mediation, gut microbiome
Citation: Hou T, Dai H, Wang Q, Hou Y, Zhang X, Lin H, Wang S, Li M, Zhao Z, Lu J, Xu Y, Chen Y, Gu Y, Zheng J, Wang T, Wang W, Bi Y, Ning G and Xu M (2023) Dissecting the causal effect between gut microbiota, DHA, and urate metabolism: A large-scale bidirectional Mendelian randomization. Front. Immunol. 14:1148591. doi: 10.3389/fimmu.2023.1148591
Received: 20 January 2023; Accepted: 13 March 2023;
Published: 30 March 2023.
Edited by:
Alexander Chouker, LMU Munich University Hospital, GermanyCopyright © 2023 Hou, Dai, Wang, Hou, Zhang, Lin, Wang, Li, Zhao, Lu, Xu, Chen, Gu, Zheng, Wang, Wang, Bi, Ning and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Xu, della.xumin@shsmu.edu.cn
†These authors have contributed equally to this work